

Summary
The field of cardiovascular (CV) imaging is facing challenges, such as high growth rates in usage resulting in increased costs and, in many cases, a lack of demonstrable utility. This article discusses emerging trends and challenges in CV imaging.
- Imaging Modalities
- Cardiac Imaging Techniques
Among the 12 million cardiovascular (CV) imaging studies that are performed each year, many are used to assess patient risk and guide patient management decisions regarding medical therapy and revascularization. Ideally, decisions regarding diagnosis, risk stratification, and treatment are made on the basis of extensive clinical evidence. However, the field of CV imaging is facing challenges, such as high growth rates in usage resulting in increased costs and, in many cases, a lack of demonstrable utility. Leslee Shaw, MD, Emory University School of Medicine, Atlanta, Georgia, USA, discussed emerging trends and challenges in CV imaging.
Dr. Shaw and colleagues recently examined several trends in the use of CV imaging modalities [Shaw LJ et al. JACC Cardiovas Imaging 2010]. With rapid and continued growth over the past decade, cardiac imaging now accounts for $80 billion in annual health care costs. In 1998, 26% of cardiology office visits included an order for cardiac imaging. By 2008, this number increased to 30% among patients aged 45 to 64 years and increased to 36% among patients aged 65 years or older. Several factors have contributed to the expanded use of CV imaging, including:
-
Increasing consumer demands
-
The growing supply of new imaging technologies
-
An aging population with more functional limitations
-
New consensus guidelines recommending the use of diagnostic imaging
-
Changes in practice patterns, such as more aggressive treatment of elderly patients
-
Increasing availability of comprehensive health care coverage
Despite the increased utilization of imaging services, cardiac imaging is poorly supported by clinical evidence in many cases. For instance, current guidelines for identifying candidates for cardiac catheterization recommend risk assessment and noninvasive testing. However, precatheterization imaging studies provide little guidance on the optimal management of patients with high-risk ischemia. In a study of 398,978 patients in the American College of Cardiology National Cardiovascular Data Registry, 83.9% underwent noninvasive testing prior to elective catheterization [Patel MR et al. N Eng J Med 2010]. Among patients without known disease, noninvasive testing was able to identify obstructive coronary artery disease (CAD) in only 37.6%. In addition, more than half (59%) of patients with positive stress test results had no obstructive CAD upon assessment with invasive angiography. Thus, in this large patient registry, cardiac imaging was a poor tool for identifying optimal candidates for catheterization and revascularization.
Better approaches to risk assessment may improve the lives of more than 12 million patients who undergo stress imaging each year, Dr. Shaw said. The National Heart, Lung, and Blood Institute (NHLBI) has developed a strategic plan for shaping the future of CV imaging research. According to the NHLBI, new clinical studies are needed to identify ways to reduce the inappropriate use of diagnostic tests and treatments. Studies are also needed to evaluate the risks, benefits, and costs of diagnostic tests and treatments in real-world patients and clinical settings. In addition, the NHLBI urges the cardiology community to incorporate diagnostic imaging techniques into future evidence-based guidelines on the prevention, diagnosis, and treatment of cardiovascular diseases (CVD).
Future of Cardiac Imaging
Raymond J. Gibbons, MD, Mayo Clinic, Rochester, Minnesota, USA, outlined future opportunities in cardiac imaging. First, Dr. Gibbons encouraged cardiologists to be strict about applying only evidence-based approaches to cardiac imaging. In many clinical situations, the current evidence does not support the routine use of imaging studies, he said. For instance, the Predictors of Response to CRT (PROSPECT) trial revealed major technical and interpretive gaps that hinder the uniform application of imaging guidelines in daily clinical practice. The PROSPECT trial found that no single echocardiographic measure of dysynchrony reliably predicted response to cardiac resynchronization therapy (CRT), in part due to high levels of variability in echocardiographic findings [Chung ES et al. Circulation 2008]. As an example, the interobserver variability in interpreting septal-to-posterior wall motion delay during echocardiography was 72.1%. According to the PROSPECT investigators, limiting the variability in measurements is a necessary step toward improving the predictive power of common cardiac imaging studies.
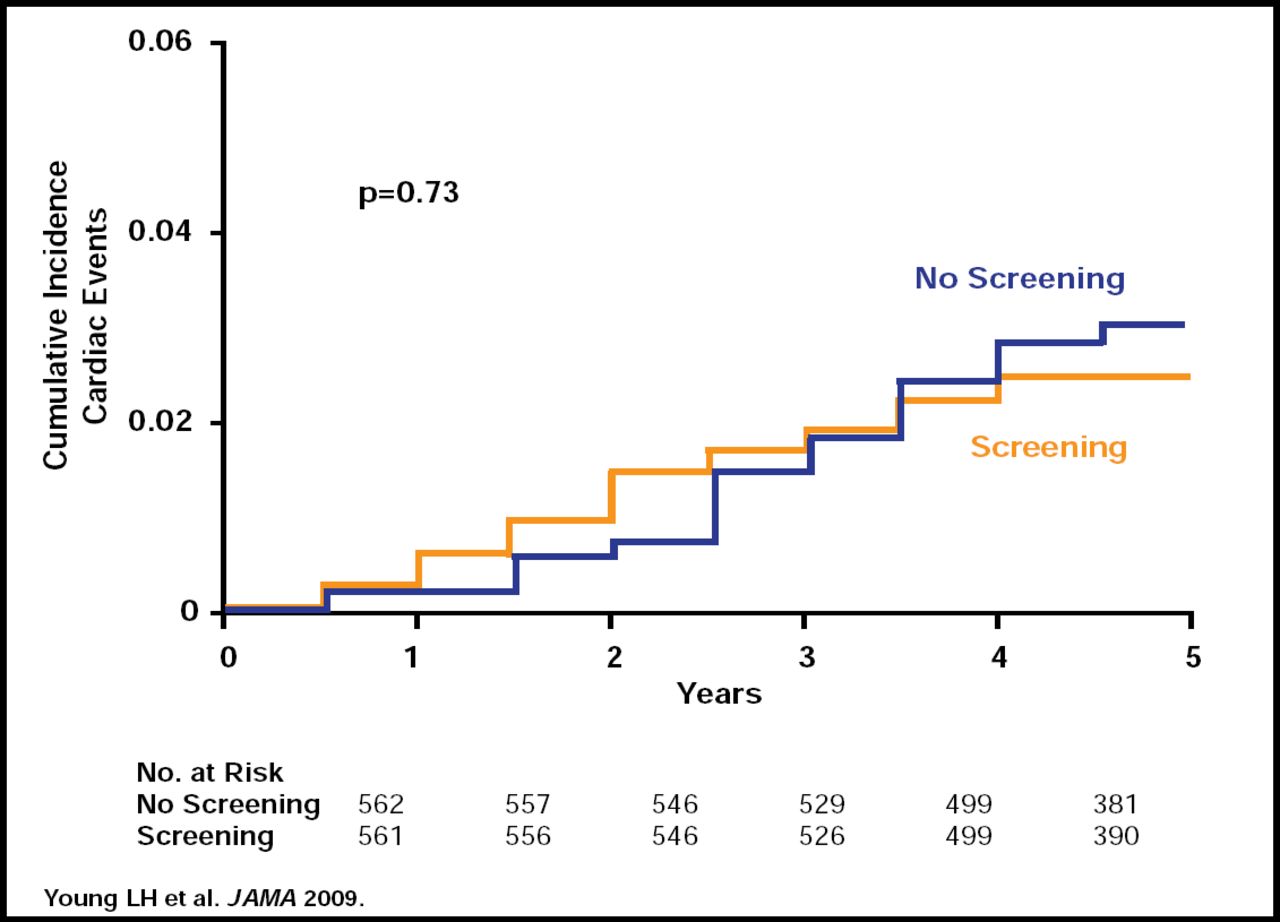
The utility of imaging modalities, such as adenosinestress radionuclide myocardial perfusion imaging (MPI), is also limited for identifying early CV risk in some patient groups. In the Detection of Ischemia in Asymptomatic Diabetics (DIAD) trial, screening for inducible myocardial ischemia with MPI did not reduce cardiac event rates among patients with diabetes [Young LH et al. JAMA 2009]. After 4.8 years, 2.7% of patients who underwent MPI screening and 3.0% of patients who were not screened developed cardiac events, including nonfatal myocardial infarction (MI) and cardiac death (p=0.73; Figure 1). Therefore, the DIAD investigators concluded that current MPI techniques do not provide enough information about ischemic risk to justify widespread screening of asymptomatic diabetic patients.

DIAD: Cardiac Event Rates With and Without Screening for Myocardial Ischemia.
Copyright © 2009 American Medical Association. All rights reserved.
Regarding the safety of current imaging tests, Dr. Gibbons recommended that clinicians balance the small risk of diagnostic radiation exposure against the potential benefit of cardiac imaging. In a recent study, Gerber and colleagues examined the lifetime cancer risk that was associated with various levels of radiation exposure [Gerber TC et al. JACC Cardiovasc Imaging 2010]. For instance, among women aged 40 to 80 years, the overall risk of cancer increases substantially with increasing age.
By comparison, annual exposure to myocardial imaging with sestamibi 25 mCi over 4 decades increases lifetime cancer risk only negligibly, suggesting that annual diagnostic radiation exposure is relatively safe. Indeed, exposure to background environmental radiation levels, which measure approximately 3 mSv per year, carries a higher potential risk of malignancy than annual sestamibi exposure (25 mCi) [Gerber TC et al. JACC Cardiovasc Imaging 2010].
Lastly, Dr. Gibbons emphasized the importance of applying appropriateness criteria to imaging studies, such as single-photon emission computed tomography (SPECT) MPI. In a retrospective review of stress testing indications in one medical center, 14% of stress SPECT MPI studies and 18% of stress echocardiography studies were performed for inappropriate reasons [Carryer DJ et al. Am Heart J 2010]. Updated appropriateness criteria from the American College of Cardiology Foundation and the American Society of Nuclear Cardiology provide important guidance on the use of SPECT MPI and other imaging studies in the clinical setting [Gibbons RJ et al. J Am Coll Cardiol 2008].
In summary, Dr. Gibbons urged the cardiology community to develop new clinical evidence that clarifies the optimal use of various cardiac imaging modalities in patients with CAD. New technologies should keep patient radiation exposure as low as possible, and cardiologists should use imaging only when the potential benefit outweighs the potential for risk. To improve the quality of cardiac care, medical centers should also strive toward reducing the inappropriate use of imaging studies, Dr. Gibbons said.
- © 2010 MD Conference Express
Tools









{kind=link}
Cited By...
- No citing articles found.