

Summary
Based on the results of the Acetylcysteine for the prevention of Contrast-Induced nephropathy [ACT; NCT00736866] trial, there is no evidence that the antioxidant N-acetylcysteine reduces the risk of contrast-induced nephropathy in patients who are undergoing coronary and vascular angiography.
- Interventional Techniques & Devices Clinical Trials
Based on the results of the Acetylcysteine for the prevention of Contrast-Induced nephropathy (ACT; NCT00736866) trial, there is no evidence that the antioxidant N-acetylcysteine (NAC) reduces the risk of contrast-induced nephropathy (CIN) in patients who are undergoing coronary and vascular angiography. That was the message from Otavio Berwanger, MD, PhD, Hospital do Coração, São Paulo, Brazil, after he presented the main results of the ACT trial.
The study was designed to test the hypothesis that using NAC could reduce the risk of CIN (defined as a ≥25% elevation in serum creatinine above baseline 48 to 96 hours postangiography) in patients who were undergoing coronary and vascular angiography. Secondary outcomes included mortality, the need for dialysis, cardiovascular mortality, side effects, and doubling of serum creatinine. CIN occurs in between 9% and 38% of patients with risk factors, such as renal failure, diabetes, and age >70 years [McCullough PA et al. Am J Card 2006]. Although there have been no large, randomized, placebo-controlled trials that have been designed to test the benefit of NAC on CIN risk, its use has become widespread.
ACT enrolled 2308 patients with at least one risk factor for CIN (ie, age >70 years, chronic renal failure, diabetes, heart failure or left ventricular ejection fraction <45, shock). The patients were randomized to receive NAC 1200 mg twice daily (2 doses pre- and 2 doses postprocedure) or placebo and underwent intravascular angiography at 46 centers in Brazil. The mean patient age was 68 years, 61% were diabetic, and the mean volume of contrast that was delivered was 100 cc.
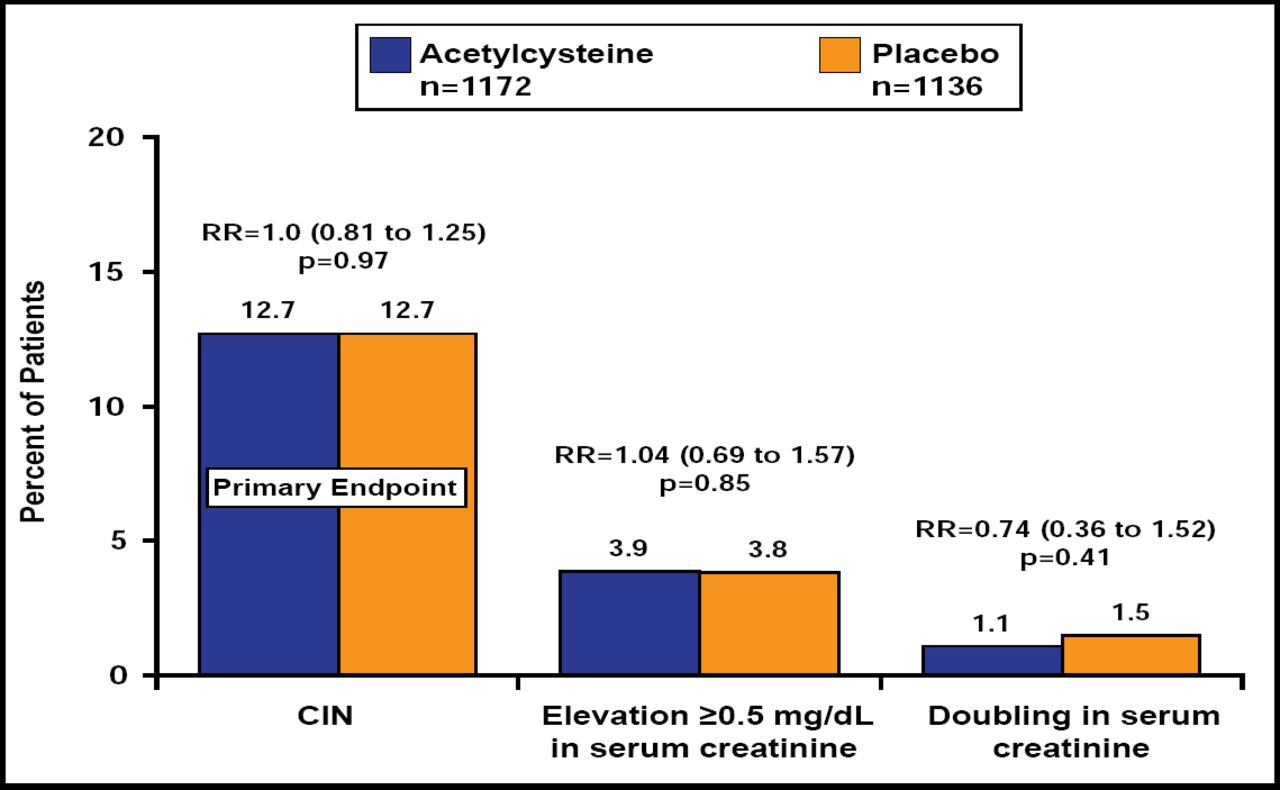
The incidence of CIN was 12.7% in both the NAC and placebo groups (RR, 1.00; 0.81 to 1.25; p=0.97; Figure 1), with nearly identical rates of mortality or the need for dialysis (2.2% vs 2.3%; p=0.91), total mortality (2% vs 2.1%; p=0.80), need for dialysis (0.3% for both; p=0.97), and cardiovascular mortality (1.5% vs 1.6%; p=0.93). The findings were consistent regardless of the type of contrast that was used for the procedure or the procedure itself (67% coronary diagnostic angiographies, 29% percutaneous interventions, 4% vascular procedures).

CIN and Serum Creatinine Increase.
Reproduced with permission from O. Berwanger, MD, PhD.
The ACT II trial, currently in the planning stages, is designed to compare saline with bicarbonate and to investigate different types of contrast dye in the search to find one that is less toxic to the kidneys or to find another compound that offers a protective effect.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.