

Summary
This article discusses a conceptual framework for a stroke system of care, STEMI systems of care, as well as cardiac resuscitation systems of care.
- Cerebrovascular Disease
- Myocardial Infarction
Evolution of an Idea
When the benefits of antithrombotic therapy first became clear in 1995, fewer than 3% of patients were receiving this therapy [Rymer MM et al. Neurol Res 2005]. The problem was not related to lack of efficacy data, acceptance, or readiness but from a need to focus on the cycle of care delivery and to create a conceptual framework for a stroke system of care, said Lee H. Schwamm, MD, Harvard Medical School, Boston, Massachusetts, USA.
Toward that end, in 2003, the American Heart Association (AHA) launched the Get-With-The-Guidelines-Stroke (GWTG-S) program; in 2004, the AHA and the Joint Commission launched the Primary Stroke Center Certification Program; and in 2005, the AHA and the American Stroke Association released recommendations for stroke systems of care. Today, 8 of 15 core Joint Commission measures for hospitals are related to stroke.
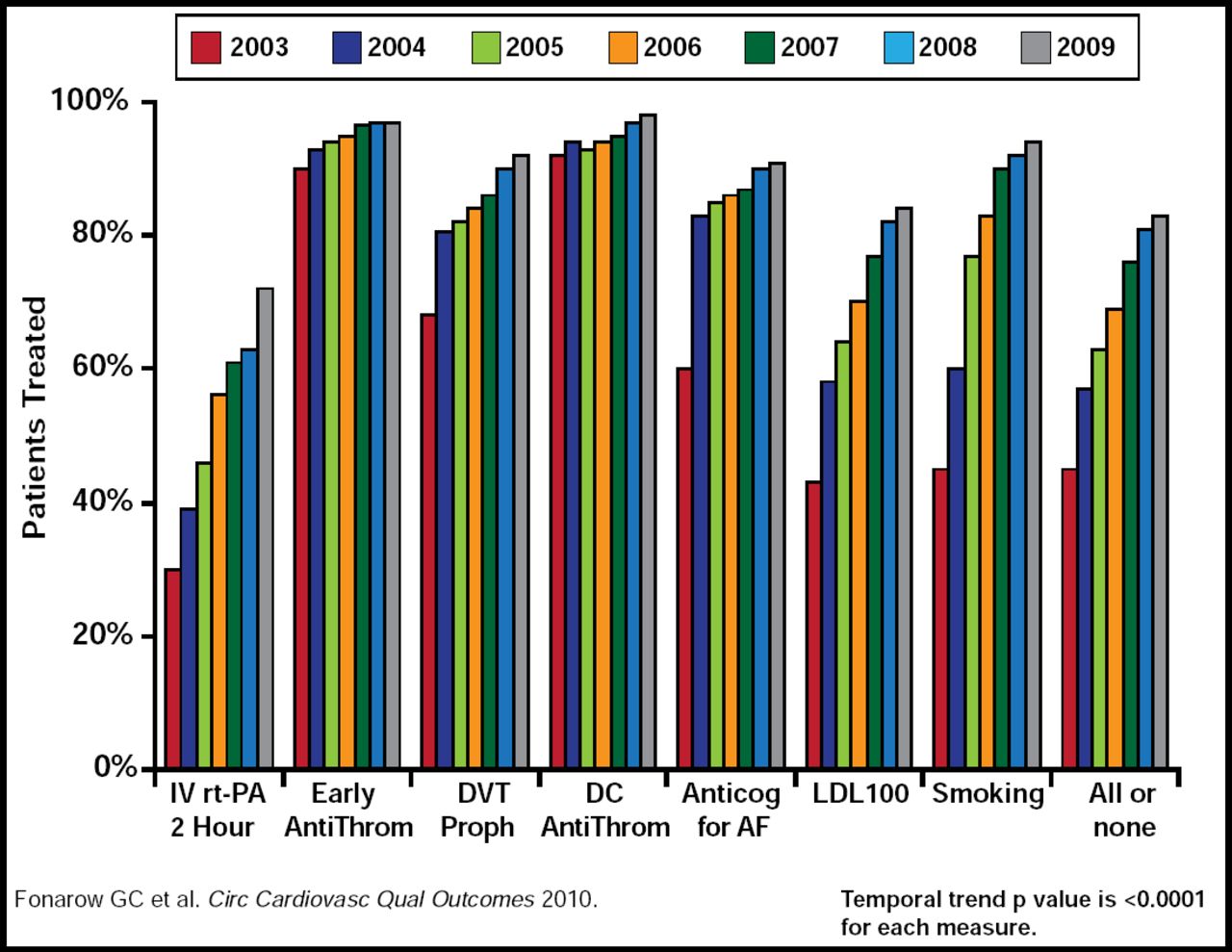
These efforts have resulted in significant improvements in quality of care (Figure 1) [Fonarow GC et al. Circ Cardiovasc Qual Outcomes 2010]. More than 80% of the United States (US) population is now within a 60-minute drive of a primary stroke center, and 86% is within a 60-minute drive of an award-winning, performance achievement GWTG-S hospital [Joint Commission Primary Stroke Centers and State-Designated Stroke Centers 2009]. In addition, there has been a significant decline in mortality from ischemic and hemorrhagic stroke since the GWTG-S program began capturing data [Joint Commission Primary Stroke Centers and State-Designated Stroke Centers 2009].

Temporal Trends in Acute Stroke and TIA Care 2003–2009.
Copyright © 2010 American Heart Association. All rights reserved.
Significant needs remain, however, Dr. Schwamm said. These include creating and implementing metrics to measure the success of the system itself and examining regional best practices to foster rapid cycle innovation. In addition, it is important to look to other industries for insight into managing and organizing teams and changing behavior and to incorporate affordability for patients and long-term sustainability into the model.
STEMI Systems of Care
The disconnect between evidence-based, life-saving, guideline-recommended therapies and the ability to deliver these therapies to all patients at all times in all places was the impetus for the development of ST-elevation myocardial infarction (STEMI) quality improvement efforts and systems of care, said Alice K. Jacobs, MD, Boston University Medical Center, Boston, Massachusetts, USA [Dougherty D et al. JAMA 2008].
In 2003, for example, 30% of STEMI patients did not receive reperfusion therapy, even in the absence of contraindications, and only a minority of those who were treated received therapy within 30 minutes (Figure 2) [McNamara RL et al. J Am Coll Cardiol 2006]. According to ACTION Registry-GWTG data from July 1, 2009 to June 30, 2010, 90% of STEMI patients who were brought directly to a PCI-equipped hospital received PCI within 90 minutes or less, while less than one-third of patients who were transferred to non-PCI-equipped care, met this important timeline goal.

Temporal Trends in ACC/AHA Guideline Adherence.
According to Dr. Jacobs, there are two model systems of STEMI care. One involves use of pre-hospital electrocardiograms and destination protocols allowing for the pre-hospital diagnosis of STEMI and direct transfer to a PCI-capable hospital. The other is the “treat and transfer” model where STEMI patients presenting to hospitals without PCI capability are rapidly treated according to ACC/AHA guidelines and transferred to a PCI-capable hospital. However, barriers to widespread implementation of STEMI systems exist. To overcome these barriers, the AHA developed Mission Lifeline: a community-based, national initiative that is designed to improve the quality of care and outcomes in patients with STEMI. It addresses the continuum of care for STEMI patients, from entry into the system through emergency medical services (EMS) to PCI Referral Hospitals (without PCI capability) to PCI-Receiving hospitals (with PCI capability) to discharge and beyond.
To understand the current status of pre-hospital STEMI care and EMS, Mission Lifeline surveyed more than 5000 EMS systems around the just country. According to Dr. Jacobs, the results show that only 58% of ambulances carry 12-lead ECGs and fewer have personnel that are trained to interpret them. In addition, 60% of regions give interhospital transfers the same priority as 911 patients, and about 40% take patients to the most appropriate facility. These percentages are lower in rural areas. According to the survey, only 51% of the US population is covered by a STEMI system.
Future plans to improve STEMI care include national certification, which will incorporate a recognition program that is modeled after the AHA GWTG program, in which hospitals are rewarded for meeting certain achievement measures. Certification criteria have been developed for entire systems, as well as for each system component.
Cardiac Resuscitation Systems of Care
Out-of-hospital cardiac arrest (OHCA) is the third leading cause of death in the US, according to data that have been extrapolated from the Centers for Disease Control and Prevention and from Resuscitation Outcomes Consortium Investigators. “We have to do better,” said Graham Nichol, MD, University of Washington, Seattle, Washington, USA. An analysis found a 500% variation in survival after EMS-treated cardiac arrest as well as a wide variation in survival from hospital admission to 1 month following cardiac arrest [Nichol G et al. JAMA 2008; Herlitz J et al. Resuscitation 2006]. Even more concerning, an analysis that was published this year found no change in OHCA survival, which remains 7.6% [Sasson C et al. Circ Cardiovasc Qual Outcomes 2010]. Given that cardiac arrest is a treatable condition, Dr. Nichol said, there is clearly a need for improved quality of care.
Furthermore, an analysis of 15,559 patients found that transporting patients to a distal, dedicated center did not negatively affect survival and that witnessed arrest, bystander-provided CPR, type of arrythmia, and EMS response time were all correlated with survival [Spaite DW et al. Ann Emerg Med].
Implementing the 2005 AHA guideline recommendations regarding the optimal use of compressions, ventilations, and induced hypothermia in the field can improve survival. A study in Wake County, North Carolina, USA, for example, found a 7.3% increase in survival overall (95% CI, 3.7 to 10.9) when impedance threshold devices were employed. A 27% increase in survival was observed when the arrest was witnessed (95% CI, 13.6 to 40.4) [Hinchey PR et al. Ann Emerg Med. 2010]. Another study found that greater survival after cardiac arrest tends to be associated with a greater volume of patients who are transported to a receiving hospital [Callaway CW et al. Resuscitation 2010]. Earlier this year, the AHA released its first policy statement on regional systems of care for OHCA, using as its rationale the impact that regionalized care has had on outcomes for patients with STEMI and life-threatening traumatic injury [Nichol G et al. Circulation 2010. Erratum in: Circulation 2010]. The statement defines these regional systems as an interconnected community, EMS, and hospital response to OHCA that is coherently organized to improve processes and outcomes in a region.
Looking Toward the Future
The next frontier for the AHA's quality initiatives will be to provide real continuity of care from primary to secondary prevention, said Rose Marie Robertson, MD, AHA Chief Science Officer. This initiative will be a joint effort with the American Cancer Society and the American Diabetes Association to complete the AHA's suite of quality improvement programs.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.