

Summary
Cardiovascular disease (CVD) is the primary cause of morbidity and mortality in people with diabetes, accounting for 70% of all deaths [Lloyd-Jones D et al. Circulation 2009]. Individuals with diabetes experience an enhanced atherosclerotic process, resulting in an increased plaque burden that affects smaller blood vessels, an increased necrotic core within the plaque, and greater macrophage and T-cell infiltration, all of which increase plaque vulnerability to rupture and result in thrombosis [Ross R et al. N Engl J Med 1999].
- Lipid Disorders
- Diabetes Mellitus
Cardiovascular disease (CVD) is the primary cause of morbidity and mortality in people with diabetes, accounting for 70% of all deaths [Lloyd-Jones D et al. Circulation 2009]. Individuals with diabetes experience an enhanced atherosclerotic process, resulting in an increased plaque burden that affects smaller blood vessels, an increased necrotic core within the plaque, and greater macrophage and T-cell infiltration, all of which increase plaque vulnerability to rupture and result in thrombosis [Ross R et al. N Engl J Med 1999].
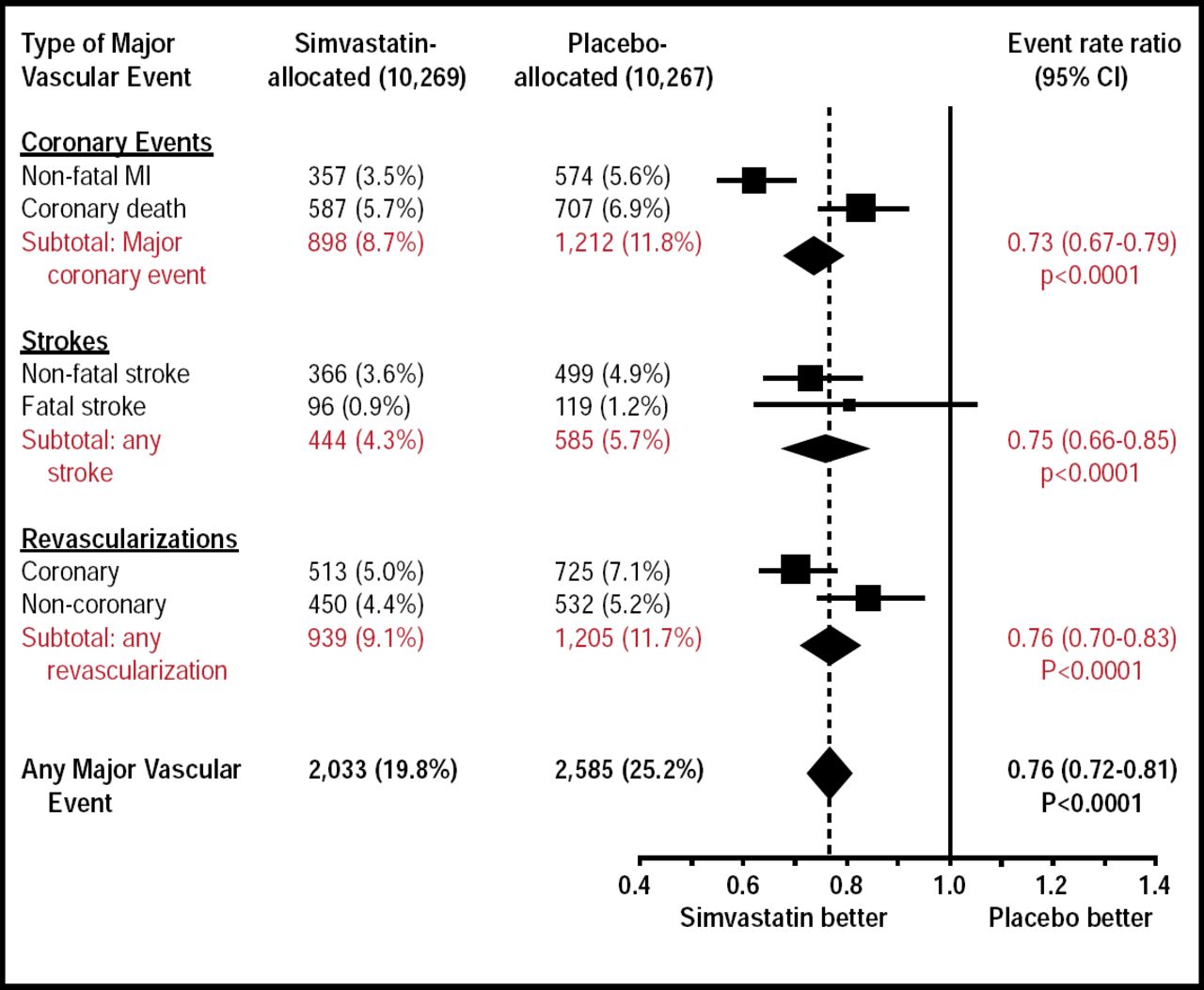
As in individuals without diabetes, HMG-CoA reductase inhibitors (statins), provide significant primary and secondary protection against vascular events in those with diabetes. Pivotal studies that have documented these benefits include the Heart Protection Study. In patients with diabetes with or without coronary heart disease or other CVD, those who received simvastatin 40 mg daily experienced significant reductions in their relative risk of cardiovascular (CV) events, regardless of their CV history [Collins R et al. Lancet 2002].

Heart Protection Study Diabetes Subgroups.
Reprinted from The Lancet. Volume 360, Issue 9326, The Heart Protection Study Collaborative Group, TMRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomized placebo controlled trial, pages 7–22, Copyright 2002, with permission from Elsevier.
It is also clear that statin therapy is important in primary prevention. The Collaborative AtoRvastatin Diabetes Study (CARDS) demonstrated a 37% relative risk reduction in vascular events among participants who received 10 mg of atorvastatin versus placebo (p=0.001) over 4 years, with significant risk reduction occurring as early as 18 months. It also found a nearly 50% risk reduction in stroke (95% CI, −69 to −11) [Hitman GA et al. Diabet Med 2007; Colhoun HM et al. Diabetologia 2005; Colhoun HM et al. Lancet 2004].
Numerous studies also attest to the benefits of extremely low levels of low-density lipoprotein (LDL). In a meta-analysis of trials that involved 27,548 patients with stable CVD or acute coronary syndrome (ACS), Cannon and colleagues identified a 16% odds reduction in coronary death or myocardial infarction among patients who received intensive statin therapy versus moderate therapy (p<0.0001) [Cannon CP et al. J Am Coll Cardiol 2006].
Significant reductions in LDL cholesterol can also result in atherosclerotic regression in patients with diabetes. In A Study to Evaluate the Effect of Rosuvastatin on Intravascular Ultrasound-Derived Coronary Atheroma Burden (ASTEROID), intensive statin therapy with rosuvastatin 40 mg daily reduced LDL cholesterol from a mean of 130.4 mg/dL to 60.8 mg/dL, resulting in significant regression in 3 primary parameters of atherosclerosis (p<0.001) [Nissen SE et al. JAMA 2006].
HDL and Triglycerides as Targets in Type 2 Diabetes Mellitus
While the risk of CVD from increased LDL level is significant in patients with diabetes, it is becoming clear that the risk is also related to low levels of high-density lipoprotein (HDL) and high levels of triglycerides (TG), even in individuals with normal LDL. This pattern of mixed dyslipidemia is particularly common among diabetics. Not only does it increase the risk of macrovascular events, it also increases microvascular consequences, such as diabetic neuropathy and retinopathy, neither of which is affected by LDL levels [Assmann G et al. Diab Vasc Dis Res 2010; Assmann G et al. Eur J Clin Invest 2007; Fioretto P et al. Nat Rev Endocrinol 2010].
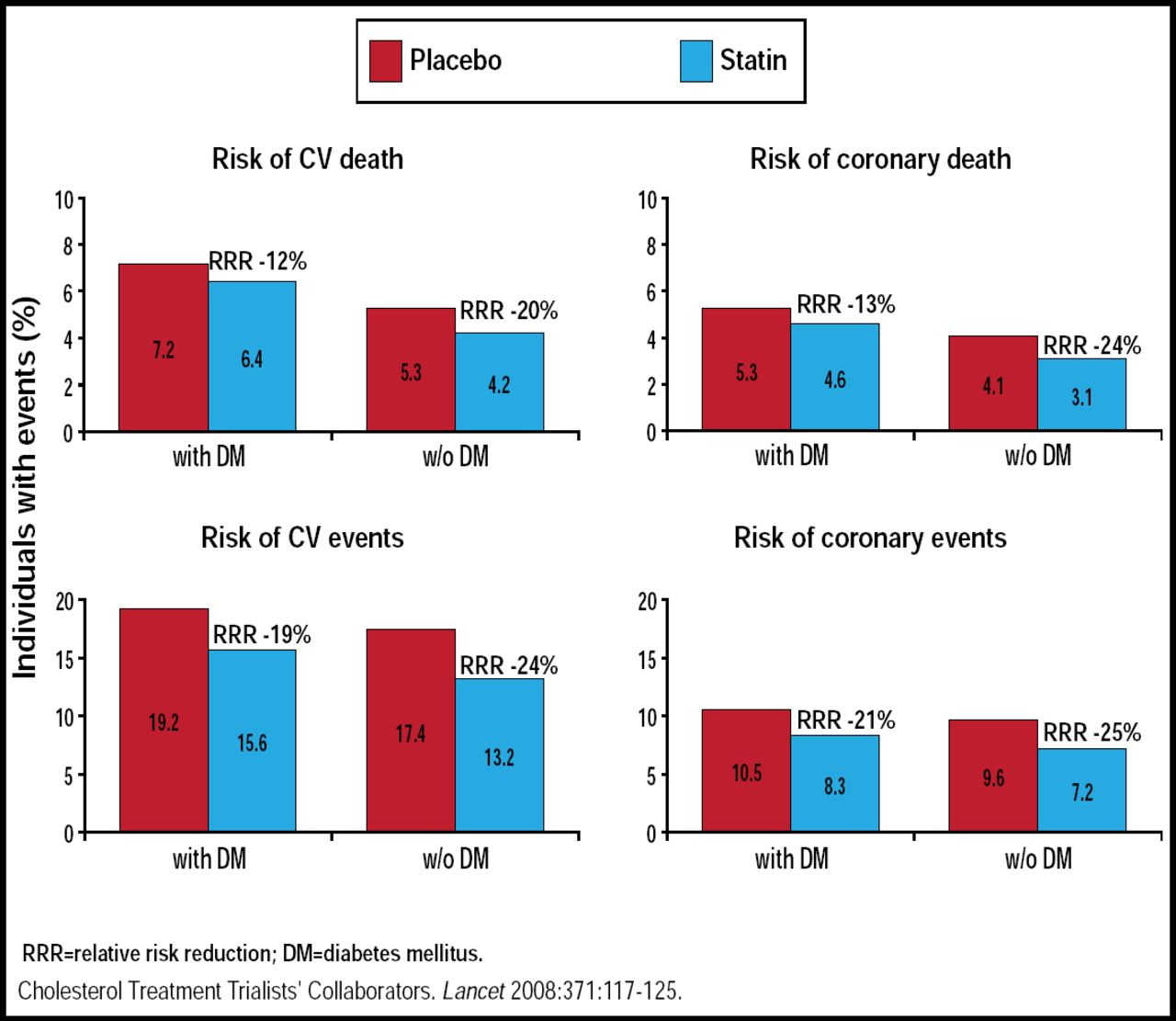
While statins are quite successful in reducing macrovascular events in patients with diabetes, they have little impact on the risk for microvascular events [Fioretto P et al. Nat Rev Endocrinol 2010]. In addition, even with their effectiveness in preventing CVD, patients with diabetes still maintain a higher risk of CV events and deaths than those without the disease (Figure 2) [Kearney PM et al. Lancet 2008]. Thus, there is a need to address other components of diabetic dyslipidemia.

Risk of CV Events and Deaths in Statin-Treated Patients With or Without Diabetes Mellitus.
Reproduced with permission from A. von Eckardstein, MD.
Unfortunately, the effect of statins on HDL and TG is also limited [Jones P et al. Am J Cardiol 1998]. Thus, other interventions are required. One option is fenofibrate. However, in the Action to reduce Cardiovascular Risk in Diabetes (ACCORD) trial, patients who were randomized to simvastatin and fenofibrate demonstrated no improvement in CV events compared with those who were randomized to simvastatin and placebo [Ginsberg HN et al. N Engl J Med 2010]. A later subgroup analysis found significant benefits in patients with elevated triglycerides (>204 mg/dL) and extremely low HDL levels (≤34 mg/dL) [Ginsberg HN et al. N Engl J Med 2010]. This subgroup accounted for 17% of patients in the ACCORD trial. Also, in other fibrate trials, patients with both low HDL cholesterol and elevated triglycerides were found to benefit from treatment with fenofibrate, bezafibrate, or gemfibrozil [Fruchart et al. Curr Med Res Opin 2010]. The message from these findings is that while it may not be appropriate to treat the entire population of patients who have HDL and TG abnormalities with fibrates, it may be appropriate for a subpopulation.
Even fibrates are limited in their ability to affect HDL. Currently, there are no approved options for increasing HDL, although the cholesterol-ester transfer protein (CETP) inhibitors that are now in clinical trials offer some potential. Phase II trials of the CETP inhibitor dalcetrapib demonstrated significant reductions in CETP activity compared with placebo in patients with and without type 2 diabetes and/or metabolic syndrome (p<0.0001 for both) [Devi L et al. PLoS One 2010].
As drugs that target HDL are introduced to clinical practice, it will be important to understand how best to use them. For instance, while lower is better in terms of risk prevention with LDL cholesterol, higher is not necessarily better when it comes to HDL levels, as indicated by a meta-analysis that was published in 2009, revealing a flattening of the benefit beyond current recommended levels [Di Angelantonio E et al. JAMA 2009].
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.