

Summary
This article discusses updated recommendations for the Standards of Medical Care for Diabetes [Diabetes Care 2010] by the American Diabetes Association. These recommendations include revised screening guidelines; revised diagnostic criteria for intermediate hyperglycemia and diabetes, both of which include suggested glucose values during oral glucose tolerance test and for HbA1C; and guidance on which patients should be considered for treatment with metformin.
- Hyperglycemia/Hypoglycemia
- Diabetes Mellitus
The American Diabetes Association (ADA) recently issued updated recommendations for the Standards of Medical Care for Diabetes [Diabetes Care 2010]. These recommendations include revised screening guidelines; revised diagnostic criteria for intermediate hyperglycemia (IH) and diabetes, both of which include suggested glucose values during oral glucose tolerance test (OGTT) and for HbA1C; and guidance on which patients should be considered for treatment with metformin (ie, those with both impaired fasting glucose and impaired glucose tolerance, or those with HbA1C ≥6%).
The new values for the diagnosis of diabetes are:
-
HbA1C ≥6.5%, or
-
Fasting glucose ≥126 mg/dL (7.0 mmol/L), or
-
2-hour plasma glucose ≥200 mg/dL (11.1 mmol/L) during an OGTT, or
-
Random plasma glucose ≥200 mg/dL (11.1 mmol/L) in patients with classic symptoms of hyperglycemia or hyperglycemic crisis
To diagnose individuals who are at high risk for diabetes, the values are:
-
Fasting plasma glucose 100–125 mg/dL (5.6–6.9 mmol/L), or
-
2-hour glucose 75 g OGTT 140–200 mg/dL (7.8–11.0 mmol/L), or
-
HbA1C between 5.7 and 6.4%
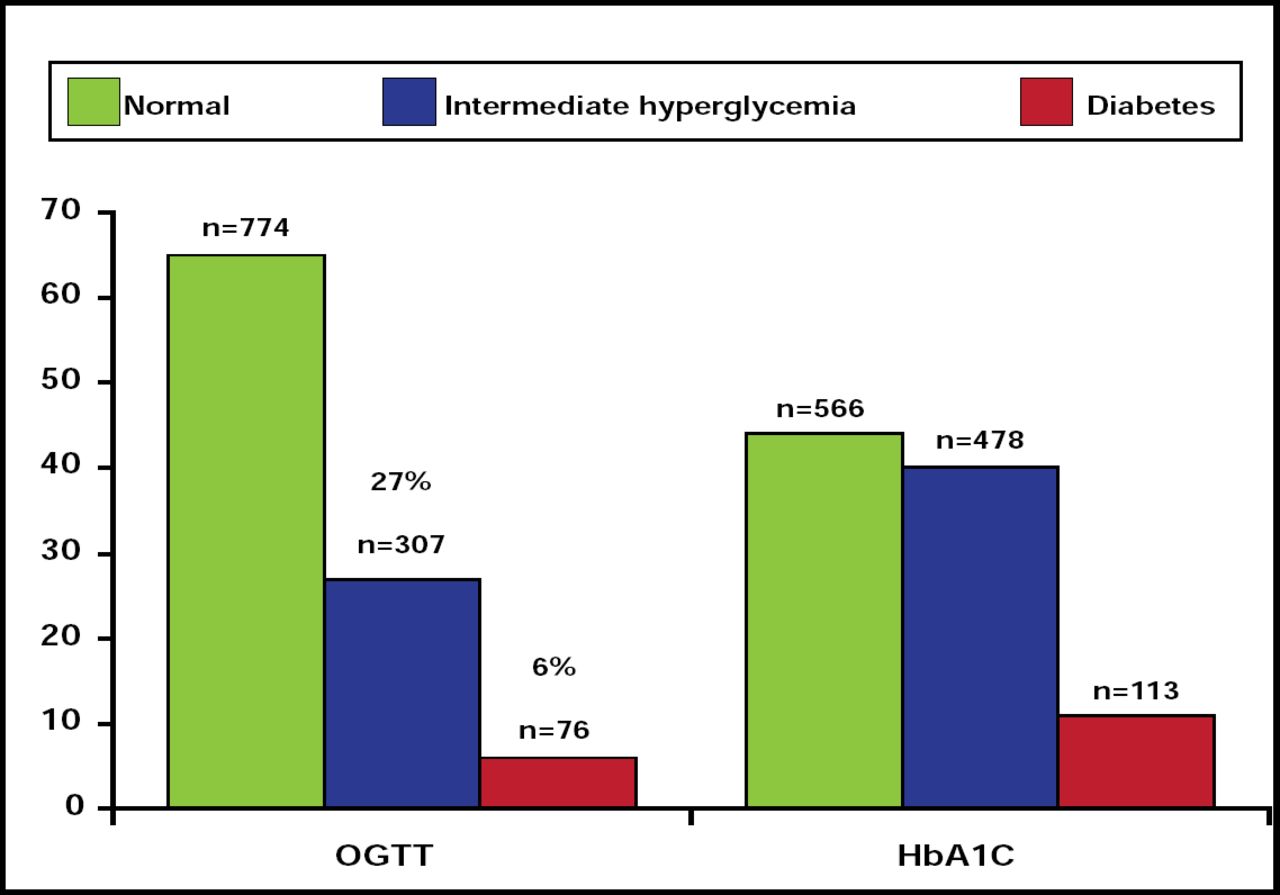
Emmaneul Cosson, MD, PhD, Paris-Nord University, Bondy, France, reported the results of a study that evaluated a diagnostic strategy using the new ADA OGTT and HbA1C criteria. The study included 1157 patients (962 women; body mass index 37.0 ± 7.2 kg/m2; mean age 41.2 ± 13.5 years) who fulfilled the new ADA screening criteria but who had not been previously diagnosed with diabetes. All participants underwent an OGTT and measurement of HbA1C. Subjects were assessed for diabetes risk (using Findrisc and DESIR scores) and coronary risk (using UKPDS score).
Use of the HbA1C strategy resulted in more patients being diagnosed with either IH (41%) or diabetes (10%) compared with the OGTT (27% and 6%, IH and diabetes, respectively; Figure 1).

Patient Diagnosis: OGTT versus HbA1C.
Reproduced with permission from E. Cosson, MD, PhD.
Based on the OGTT results, 11.2% of patients (n=130) would be eligible for treatment with metformin versus 22.0% (n=255) using the HbA1C strategy.
The sensitivity and specificity of HbA1C ≥6.5% for the diagnosis of diabetes according to the OGTT were 44.7% and 92.7%, respectively. In patients with HbA1C <6.5%, the sensitivity of HbA1C 5.7% to 6.4% for the diagnosis of IH was 57.9%, and the specificity was 59.3%. Diabetes risk score and UKPDS risk score were highest in patients with both an abnormal OGTT and HbA1C ≥5.7% (n=130).
The results of this study show that in a population that meets the new screening criteria, choosing the HbA1C strategy rather than the OGTT strategy leads to more individuals being diagnosed and more patients being treated with metformin, although the consistency of both diagnostic criteria is low (eg, 1/3 of patients with HbA1C ≥6.5% have a normal OGTT). The patients who have the highest a priori risk of diabetes and cardiovascular disease are those with an abnormal OGTT that is associated with HbA1C ≥5.7%.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.