

Summary
Long-term follow-up (up to 3 years) that compared everolimus-eluting (EES) and sirolimus-eluting stents for coronary revascularization revealed that the unrestricted use of EES was associated with lower risk of myocardial infarction, target vessel revascularization, and stent thrombosis. The Long-term comparison of Everolimus-eluting and Sirolimus-eluting Stents for cOronary revascularizatioN [LESSON-I] data are discussed in this article.
- Myocardial Infarction
Long-term follow-up (up to 3 years) that compared everolimus-eluting (EES) and sirolimus-eluting stents (SES) for coronary revascularization revealed that the unrestricted use of EES was associated with lower risk of myocardial infarction (MI), target vessel revascularization (TVR), and stent thrombosis. The Long-term comparison of Everolimus-eluting and Sirolimus-eluting Stents for cOronary revascularizatioN (LESSON-I) data were presented by Stephan Windecker, MD, Bern University Hospital, Bern, Switzerland.
LESSON-I was a nonrandomized, observational study that included 3133 patients with stable angina and acute coronary syndromes who were undergoing percutaneous coronary intervention (PCI) at Bern University Hospital. After propensity score-matching, 2684 patients were included in the analysis (1342 matched pairs), with a median clinical follow-up of 1.3 years. Patients who were undergoing SES implantation prior to April 2003 and those who were previously included in the SIRTAX trial were excluded from this study. The primary endpoint was the patient-oriented composite of death, MI, and TVR through 3 years. The secondary endpoints included death, MI, TVR, TLR, cardiac death or MI, and stent thrombosis, according to the Academic Research Consortium (ARC). Patients who were treated with EES were more complex as compared with patients who were treated with SES. Multivessel treatment was performed in 24% of patients in the EES group (average number of stents was 2.0±1.1) and 16% of patients in the SES group (average number of stents was 1.8±0.9).
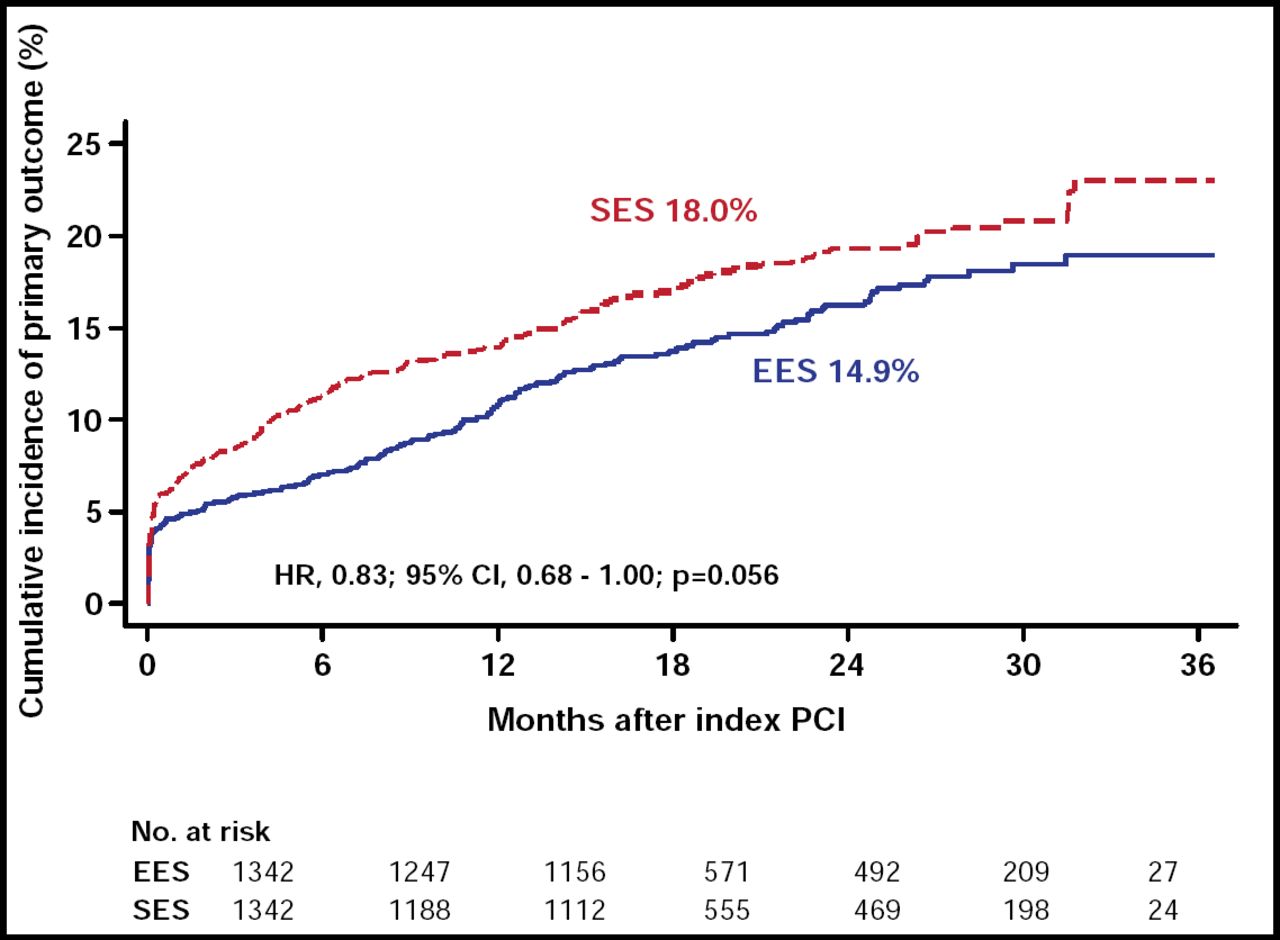
At 3 years, the rate of death, MI, or TVR was lower in the EES group than in the SES group (HR, 0.83; 95% CI, 0.68 to 1.00; p=0.056), while the rate of all-cause mortality was similar for both groups (Figure 1). The rates of MI and TVR at 3 years were significantly reduced in EES subjects as compared with SES recipients (3.3% vs 5.0% for MI; p=0.017 and 7.0% vs 9.6% for TVR; p=0.039 respectively). The incidence of definite stent thrombosis up to 3 years was lower in the EES group as well (0.5% vs 1.6% for SES; HR, 0.30; 95% CI, 0.12 to 0.75; p=0.01), and of note, not a single very late stent thrombosis occurred in the EES group. Prof. Windecker concluded that the differences in MI rates were driven by a 70% lower risk of QWMI and were present early but continued to increase during longer-term follow-up. The lower risk of MI in favor of EES was explained at least in part by the lower risk of definite stent thrombosis.

Primary Endpoint.
Reproduced with permission from L. Räber, MD.
The concept that EES was associated with lower rates of MI, partially owing to lower stent thrombosis risk, is interesting and may have clinical implications with regard to the duration of dual antiplatelet therapy. EES appears to be a safe and effective method for coronary revascularization in an all-comers population and may provide more favorable outcomes, particularly related to very late stent thrombosis, compared with SES. However, further investigation in the setting of a large-scale randomized clinical trial is needed in order to confirm these findings.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.