

Summary
Hypertension is a highly prevalent and powerful contributor to the growing worldwide burden of cardiovascular disease. Antihypertensive therapy significantly reduces the risk of cardiovascular morbidity and mortality that accompanies arterial hypertension. Despite the benefits of blood pressure reduction, approximately 70% of hypertensive adults worldwide are uncontrolled [Hajjar I et al. JAMA 2003]. This article discusses the emerging role of combination therapy in the management of difficult-to-treat hypertension.
- Hypertensive Disease
Hypertension is a highly prevalent and powerful contributor to the growing worldwide burden of cardiovascular disease (CVD). Antihypertensive therapy significantly reduces the risk of cardiovascular (CV) morbidity and mortality that accompanies arterial hypertension. Despite the benefits of blood pressure (BP) reduction, approximately 70% of hypertensive adults worldwide are uncontrolled [Hajjar I et al. JAMA 2003]. In the US, 50% of patients who receive antihypertensive therapy do not achieve BP goals [Hajjar I et al. JAMA 2003]. Undertreatment is also a major problem in Europe, where only 8% of the hypertensive population reports BP levels <140/90 mm Hg [Wolf-Maier K et al. JAMA 2003]. Charles V. Pollack, Jr., MA, MD, University of Pennsylvania, Philadelphia, Pennsylvania, USA, and Carlos M. Ferrario, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA, discussed the emerging role of combination therapy in the management of difficult-to-treat hypertension.
Options for Antihypertensive Therapy
Lifestyle modifications, including smoking cessation, weight reduction, and increased activity level, should be recommended as the first step toward hypertension management for all patients. Pharmacological treatment typically begins with monotherapy, followed by sequential monotherapy or by combination therapy in patients who do not reach BP goals. More than half of hypertensive patients will require combination therapy to lower their BP below 140/90 mm Hg. Ideally, antihypertensive agents that are used in combination therapy should be selected to maximize potential synergistic effects on BP, maintain acceptable tolerability, and minimize adverse effects.
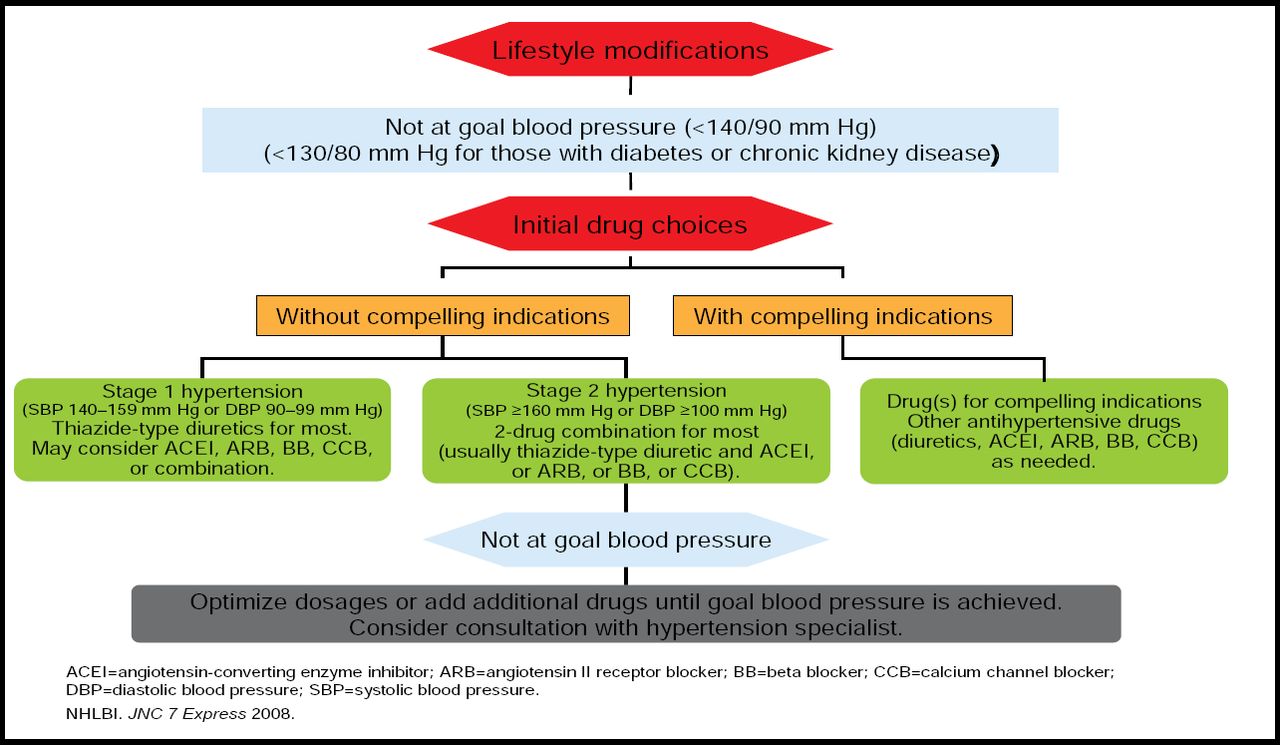
According to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7), most patients with hypertension will require two or more antihypertensive agents [Chobanian AV et al. JAMA 2003]. A second drug from a different class should be added when a single drug in adequate doses is insufficient to achieve BP goals (Figure 1). When BP is more than 20/10 mm Hg above goal, initial treatment with combination therapy should be considered. Combination therapy is also recommended by other major guidelines on hypertension treatment. The Consensus Statement of the Hypertension in African Americans Working Group of the International Society on Hypertension in Blacks (ISHIB) recommends first-line combination antihypertensive therapy for patients with a systolic BP that is 15 mm Hg or more above target or a diastolic BP that 10 mm Hg or more above target [Douglas JG et al. Arch Intern Med 2003].

JNC 7 Algorithm for the Treatment of Hypertension.
Reproduced with permission from the National Heart, Lung, and Blood Institute.
Emerging Role of Combination Antihypertensive Therapy
Combination therapy is one of the most important tools in the management of uncontrolled BP. When appropriately selected, fixed-dose combination therapies can significantly increase patient compliance, reduce side effects, and improve BP control. In a meta-analysis of 354 randomized, double-blind, placebo-controlled trials that enrolled a total of 56,000 patients with uncontrolled BP, Law and colleagues demonstrated important features of combination antihypertensive therapy [Law MR et al. BMJ 2003]. Patients were treated with thiazide-type diuretics, β-blockers, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), and/or calcium channel blockers, given alone or as part of combination therapy.
When given alone at standard doses, all five classes of antihypertensive medications yielded similar reductions in systolic (mean, 9.1 mm Hg) and diastolic (mean, 5.5 mm Hg) BP. At half-standard doses, the antihypertensive medications still provided pronounced reductions in systolic and diastolic BP (7.1 mm Hg and 4.1 mm Hg, respectively). When given in combination, the BP-lowering effects of different drugs classes were additive, but adverse events were not. Moreover, with the exception of ACE inhibitor-associated cough, all treatment-related adverse events appeared to be dose-related.
The study authors concluded that the use of combination low-dose antihypertensive therapy significantly improved treated efficacy while reducing the risk of adverse events. For a hypothetical patient aged 60 to 69 years with a baseline BP of 150/90 mm Hg, combination therapy with 2 or 3 low-dose antihypertensive agents would be preferable to treatment with 1 or 2 agents at standard dose. In this example, combination low-dose therapy could reduce BP by approximately 20/11 mm Hg, thereby reducing the lifetime risk of stroke by 63% and the risk of ischemic heart events by 46% [Law MR et al. BMJ 2003].
ARB-Based Combination Antihypertensive Therapy
In patients with hypertension, ARBs appear to have many benefits beyond BP reduction. ARBs reduce the risk of CV and cerebrovascular events. In patients with comorbid type 2 diabetes, ARBs slow the progression of renal damage and delay the onset of diabetic nephropathy. ARBs have also been shown to improve outcomes in patients with heart failure and following an acute MI. Given this range of potential benefits, there is considerable interest in incorporating ARBs into combination antihypertensive regimens.
Several recent trials have focused on evaluating the efficacy and safety of ARB-based combination regimens. The INCLUSIVE trial enrolled 1005 patients whose hypertension was uncontrolled despite treatment with a single antihypertensive agent. In this difficult-to-treat patient population, treatment with the fixed-dose combination of irbesartan and hydrochlorothiazide (HCTZ) reduced systolic and diastolic BP by 20.5 mm Hg and 10.4 mm Hg, respectively (p<0.001). After 18 weeks of therapy, 77% of patients reached the systolic BP goal of <140 mm Hg (<130 mm Hg in patients with diabetes), and 83% of patients reached the diastolic BP goal of <90 mm Hg (<80 mm Hg in those with diabetes) [Neutel JM et al. J Clin Hypertens 2005].
The RAPiHD trial demonstrated the early therapeutic benefits of first-line combination irbesartan/HCTZ therapy in patients with severe hypertension. In this patient population, nearly half (47%) of patients medicated with this combination reached the diastolic BP goal of <90 mm Hg after 5 weeks of treatment. The mean reduction in systolic and diastolic BP following 5 weeks of treatment with irbesartan/HCTZ was 30.8 mm Hg and 24.0 mm Hg, respectively. The overall adverse event rates in the irbesartan monotherapy and irbesartan/HCTZ groups were similar (8.8% vs 11.5%), suggesting no increase in adverse events with combination therapy [Neutel JM et al. J Clin Hypertens 2008].
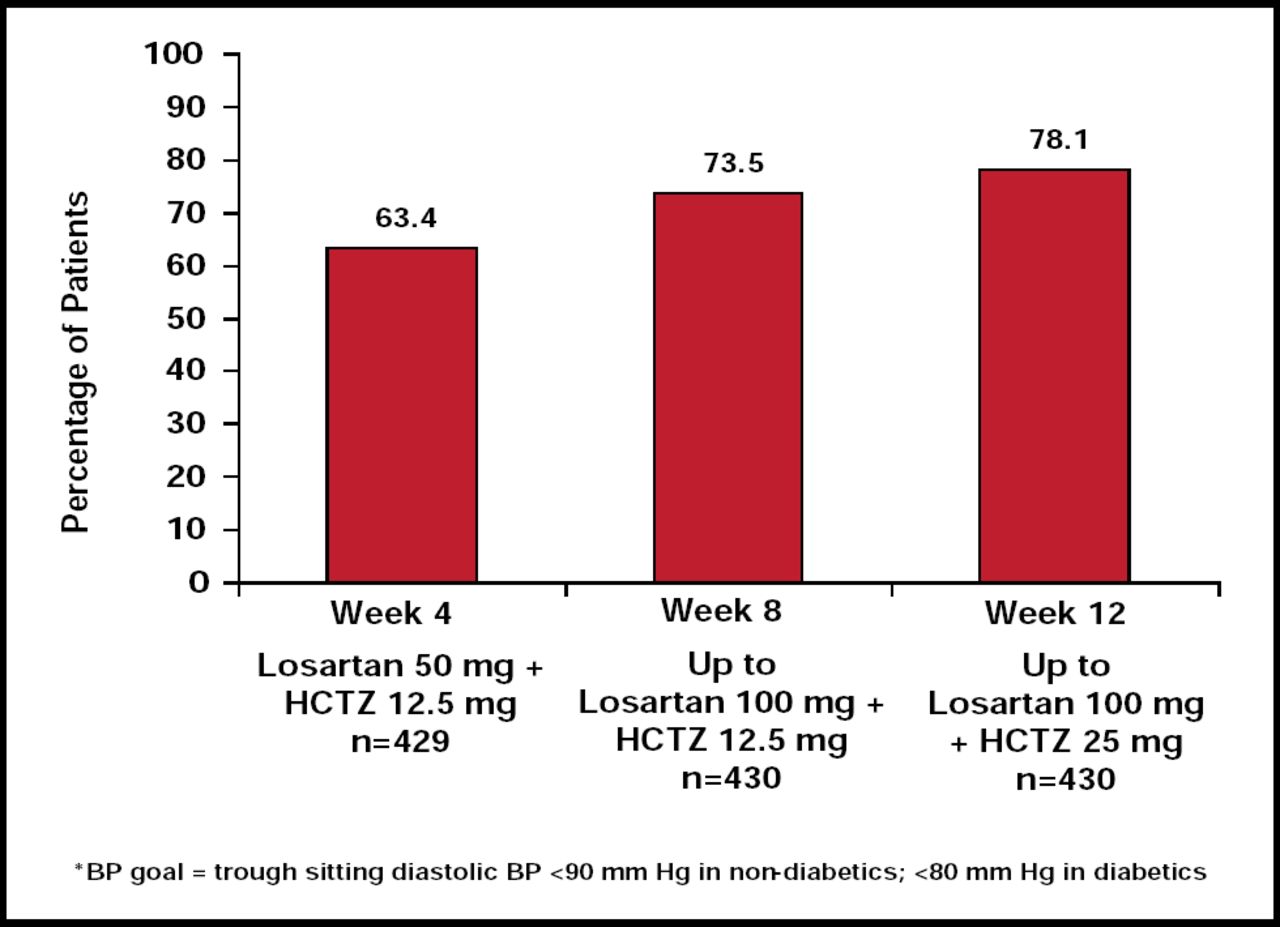
Combination therapy with losartan/HCTZ also significantly improved BP control in a study of patients with essential hypertension whose BP was uncontrolled with ACE inhibitor or ARB monotherapy [Li Y et al. Int J Clin Pract 2003]. By Week 4, 63.4% of patients reached the diastolic BP goal (<90 mm Hg for nondiabetic patients or <80 mm Hg for diabetic patients). By Week 12 of combination losartan/HCTZ treatment, 78.1% of previously uncontrolled patients had achieved BP control (Figure 2).

Percentage of Patients Reaching BP Goal.*
Reproduced with permission from C. Ferrario, MD.
In another trial by Pool and colleagues, 1346 patients with essential hypertension were randomized to 1 of 8 treatments (VAL 160 or 320 mg; HCTZ 12.5 mg or 25 mg; VAL/HCTZ 106/12.5 mg, 320/12.5 mg or 320/25 mg; or placebo). Each VAL/HCTZ combination was associated with significantly greater reductions in BP compared with placebo or with either agent given as monotherapy (p<0.001 for all). The mean reduction in mean sitting diastolic and systolic BP with VAL/HCTZ 320/25 mg compared with VAL/HCTZ 160/12.5 mg (p<0.002). The combination regimen was also well tolerated, with fewer episodes of hypokalemia than HCTZ alone [Pool JL et al. Clin Ther 2007]. In the VELOCITY trial, adverse event rates with first-line valsartan/HCTZ combination therapy were similar to those with valsartan monotherapy [Jamerson K et al. J Clin Hypertens 2007].
Additional Benefits of Combination Therapy
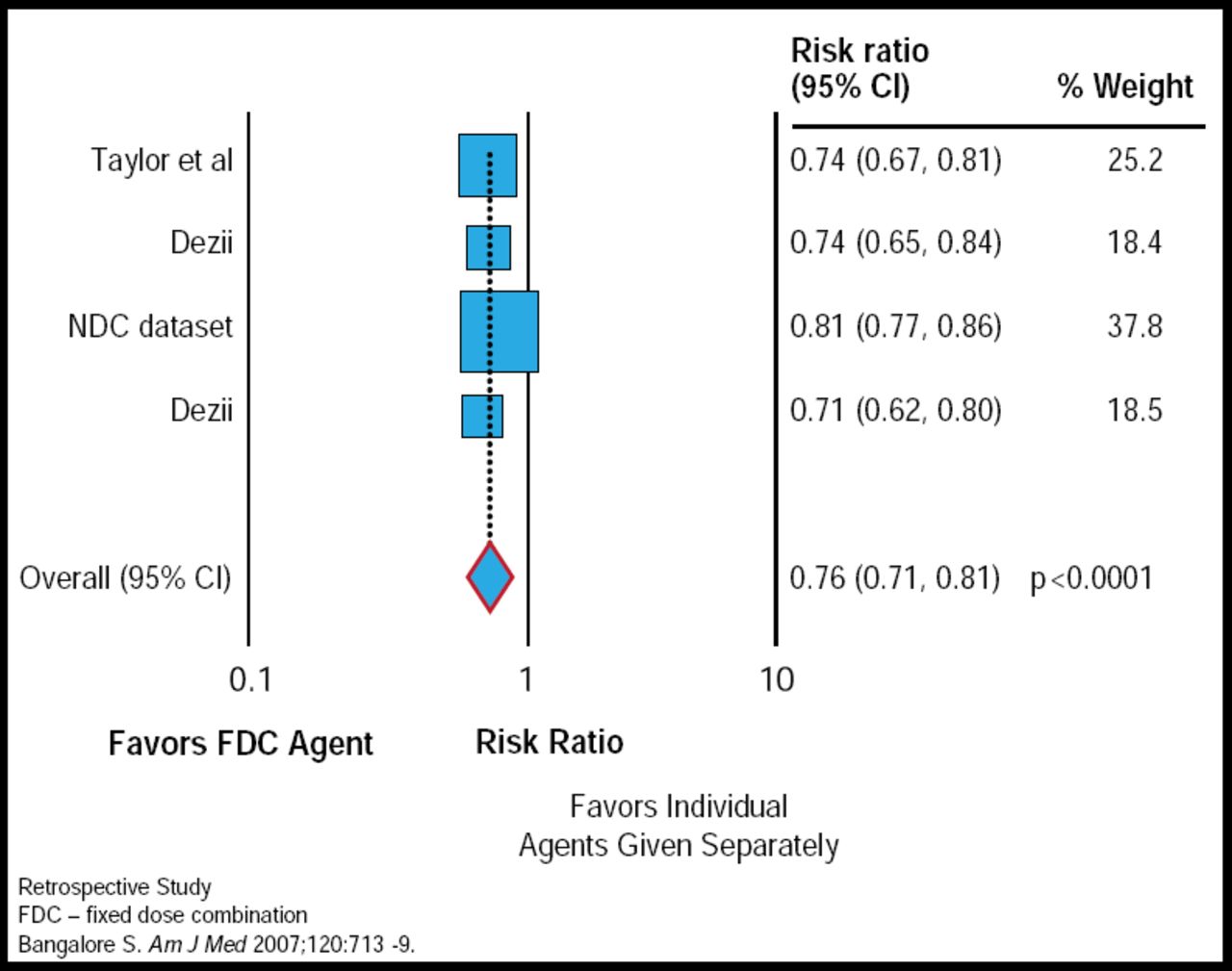
Patients with more complex antihypertensive regimens, including a higher pill burden, are less likely to adhere to therapy. A meta-analysis showed that the use of single-pill, fixed-dose combination antihypertensive therapy increased patient adherence by 23% compared with the use of the same drugs prescribed separately (p<0.0001; Figure 3) [Bangalore S et al. Am J Med 2007]. Therefore, in addition to providing superior efficacy and similar tolerability compared with single-agent antihypertensive therapy, fixed-dose combinations remove a major barrier to successful BP control.

Single-Pill Combination Therapy Demonstrates Improved Compliance.
Reprinted from the American Journal of Medicine. Vol 120(8):713–719. August 2007. Bangalore S et al. Fixed-Dose Combinations Improve Medication Compliance: A Meta-Analysis. With permission from Elsevier.
In summary, effective BP control is the main goal of antihypertension therapy. Most patients will require combination antihypertension therapy to achieve treatment targets. The initial or earlier use of combination therapy may allow patients to achieve the clinical benefits of BP reduction more quickly, with fewer adverse events and a greater likelihood of adherence, compared with single-agent treatment.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.