

Summary
Atrial fibrillation (AF) is a major public health burden that affects 7 million patients in the US and Europe, and a growing number of patients worldwide. This article discusses new treatment options for the management of patients with AF.
- Arrhythmias
Atrial fibrillation (AF) is a major public health burden that affects 7 million patients in the US and Europe, and a growing number of patients worldwide. In this session, Augustus O. Grant, MD, Duke University School of Medicine, Durham, North Carolina, USA, focused on new treatment options for the management of patients with AF.
The goals of AF therapy include symptom reduction, improvement in quality of life, prevention of stroke and systemic arterial embolism, restoration of atrial transport function, reversal of the remodeling process, reduction in hospitalizations, and prolonged survival. Several treatment options are available to help patients achieve these goals, including rate-controlling drugs, antiarrhythmic agents, and antithrombotic therapy. Some patients may also be candidates for cardiac ablation.
Treatment of AF typically begins with the selection of a rhythm control or rate control strategy. The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) trial showed that patients who were assigned to rhythm control therapy tended to have a higher 5-year mortality than those who were assigned to rate control therapy (23.8% vs 21.3%; p=0.08) [Wyse DG et al. N Engl J Med 2002]. Patients who were treated with a rhythm control strategy also had a higher risk of hospitalization (80.1% vs 73.0%; p<0.001) and were more likely to experience adverse drug effects than those who were managed with rate control therapy.
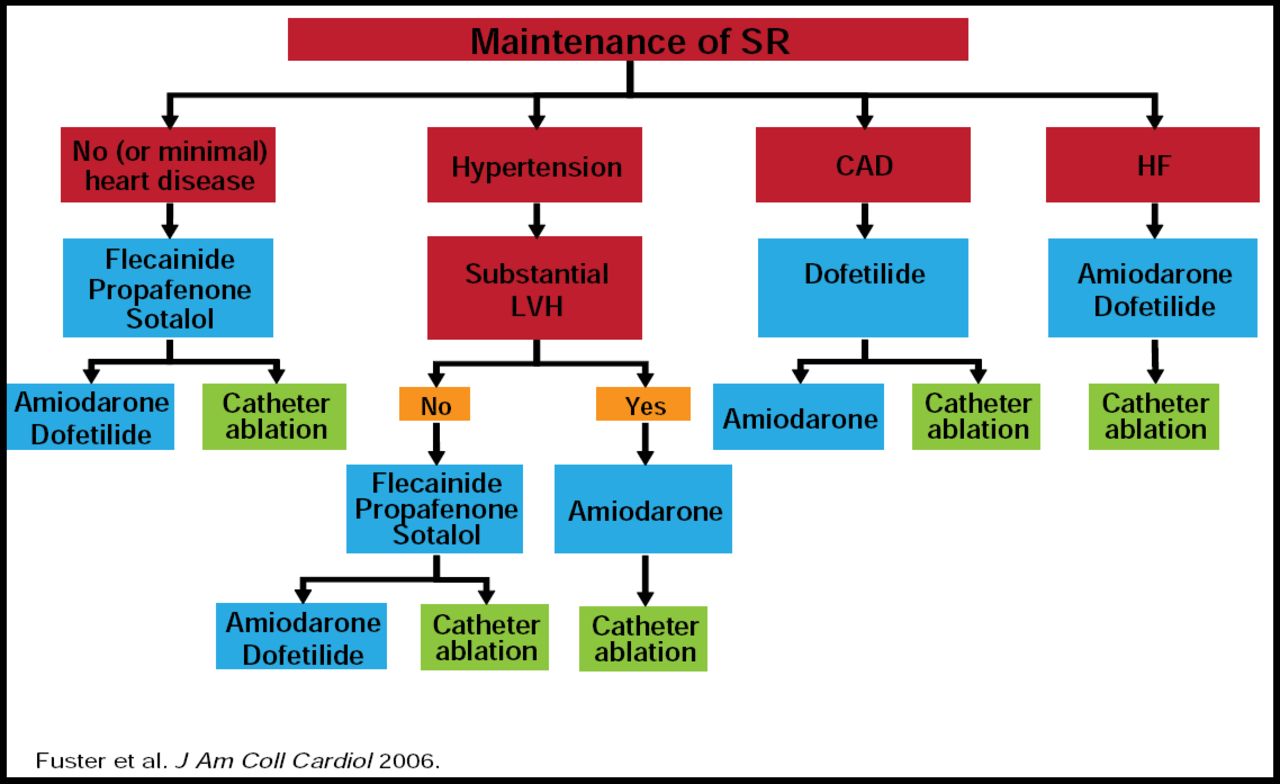
Initial treatment strategies should be adapted to the unique needs of the individual patient. The benefits of a rate control strategy may not apply to all patients with AF, particularly younger patients without heart disease, patients in whom prior rate control therapy has failed, or patients with normal left ventricular function or no risk of stroke. Current guidelines provide algorithms for antiarrhythmic use in specific clinical conditions (Figure 1) [Fuster V et al. Circulation 2006].

Options for Maintenance of Sinus Rhythm in Patients with AF.
Reproduced with permission from A. Grant, MD.
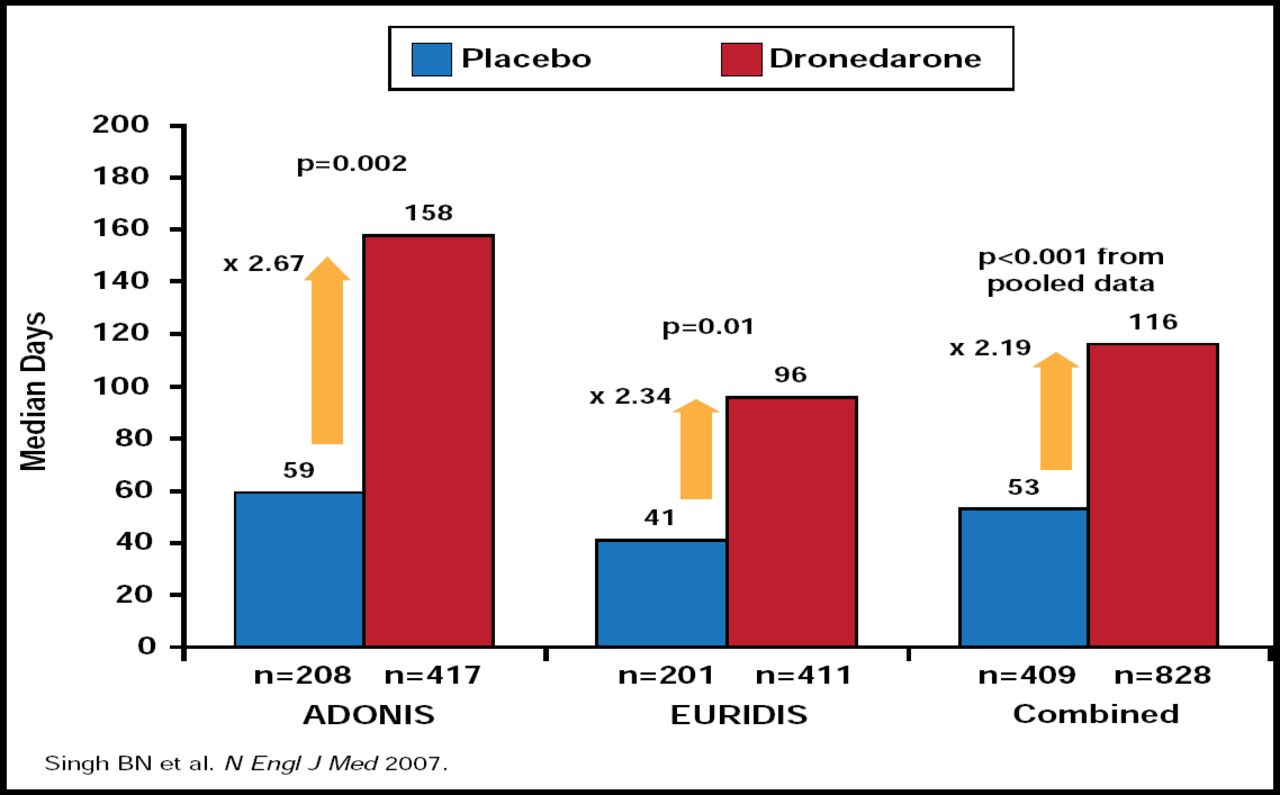
New antiarrhythmic agents provide new options for improving outcomes in the management of AF. Dronedarone is structurally similar to amiodarone but lacks the iodine moiety. This structural change allows dronedarone to provide similar electrophysiological effects but without the thyroid and pulmonary toxicity that is associated with amiodarone therapy. Data from the European Trial in Atrial Fibrillation or Flutter Patients Receiving Dronedarone for the Maintenance of Sinus Rhythm (EURIDIS) and American-Australian-African Trial with Dronedarone in Atrial Fibrillation or Flutter Patients for the Maintenance of Sinus Rhythm (ADONIS) trials, as well as pooled data from both trials, show that dronedarone significantly delays the time to first recurrence of AF or atrial flutter compared with placebo (Figure 2) [Singh BN et al. N Engl J Med 2007]. In A Placebo-Controlled, Double-Blind, Parallel Arm Trial to Assess the Efficacy of Dronedarone 400 mg bid for the Prevention of Cardiovascular Hospitalization or Death from any Cause in Patients with Atrial Fibrillation/Atrial Flutter (ATHENA), dronedarone significantly reduced the time to first cardiovascular hospitalization or death by 24% compared with placebo (p<0.001) [Hohnloser HS et al. N Engl J Med 2009].

Dronedarone Prolongs Time to First Recurrence of AF or Atrial Flutter.
Reproduced with permission from A. Grant, MD.
Stroke prevention is another important therapeutic goal for patients with AF. Vitamin K antagonists, such as warfarin, are currently the treatment of choice for the prevention of stroke in high-risk patients with AF. In the ACTIVE W trial, warfarin reduced the risk of thrombotic events without raising the risk of major bleeding compared with dual antiplatelet therapy with clopidogrel and aspirin [Connolly SJ et al. Circulation 2008]. Despite the clear benefits of warfarin therapy in stroke prevention, many patients with high-risk AF are suitable candidates for oral anticoagulation therapy due to bleeding risk, patient preference, or an inability to maintain warfarin within the therapeutic range. Therefore, patients with AF require new options for long-term stroke prevention.
Dabigatran is a novel antithrombotic agent that reversibly binds to free and fibrin-bound thrombin. In the Randomized Evaluation of Long-Term Anticoagulant Therapy (RE-LY) trial, once-daily dabigatran 150 mg reduced the risk of stroke and systemic embolism by 33% (p<0.001) compared with warfarin. The net clinical benefit, which incorporated the absence of stroke or systemic embolism, death, myocardial infarction, pulmonary embolism, and major bleeding, favored treatment with dabigatran [Connolly SJ et al. N Eng J Med 2009].
In summary, treatment options AF are expanding. New antiarrhythmic options may improve long-term cardioversion and enhance clinical outcomes in patients with AF. In addition, novel anticoagulants may reduce the risk of thrombotic events while minimizing the risk of bleeding, particularly in high-risk populations.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.