

Stroke prevention is a priority for clinicians who treat patients with atrial fibrillation (AF). Warfarin has been the gold standard therapy for patients with AF who are at moderate or high risk of stroke. However, there are concerns about the limitations of warfarin, such as adherence issues, bleeding risk, narrow therapeutic window, vigilant monitoring requirements, and drug-drug/food-drug interactions that make it difficult to manage in a clinical setting. Novel strategies for stroke prevention may replace the widespread use of warfarin in the future. One new therapy was shown to be superior to warfarin in a large clinical trial, while three others are in late-stage testing. Stephen La Haye, MD, Kingston General Hospital, Kingston, Ontario, Canada, discussed various approaches to stroke prevention in AF and their relevance to clinical practice.
In high-risk patients with AF, most strokes occur either after warfarin discontinuation in the absence of warfarin or in the presence of suboptimal international normalized ratio (INR) levels, suggesting that anticoagulation therapy should be continued in this cohort [The AFFIRM Investigators. N Engl J Med 2002; Gladstone DJ et al. Stroke 2009]. While this therapy may be indicated from an efficacy standpoint, the issue of nonadherence and other limitations must be considered, and alternative approaches are warranted. In the ACTIVE studies, investigators assessed the safety and efficacy of other agents (ie, clopidogrel plus aspirin combination therapy and irbesartan) on stroke prevention in patients with AF. In the ACTIVE-W study, comparing clopidogrel + aspirin with warfarin, oral anticoagulation therapy was found to be superior to clopidogrel + aspirin for the prevention of vascular events in high-risk patients with AF (p=0.0003) [The ACTIVE Investigators. Lancet 2006]. The ACTIVE-A study, which included patients with contraindications to warfarin or who were unwilling to take warfarin, compared clopidogrel + aspirin combination therapy with aspirin alone. Those who received combination therapy had a significantly lower rate of stroke compared with aspirin alone (RR, 0.72; 95% CI, 0.62 to 0.83; p<0.001). However, the risk of major hemorrhage was significantly higher among those who were taking clopidogrel (RR, 1.57; 95% CI, 1.29 to 1.92; p<0.001) [The ACTIVE Investigators. N Engl J Med 2009].
Dr. La Haye put these data into perspective by explaining the risk versus benefit of clopidogrel combination therapy compared with warfarin. Over the course of 3 years, 28 strokes would be prevented for every 1000 patients on clopidogrel + aspirin therapy, but 20 major nonstroke bleeds (3 fatal) would also occur (Table 1).
Risk Versus Benefit of ASA + Clopidogrel Versus Warfarin: The ACTIVE Study.
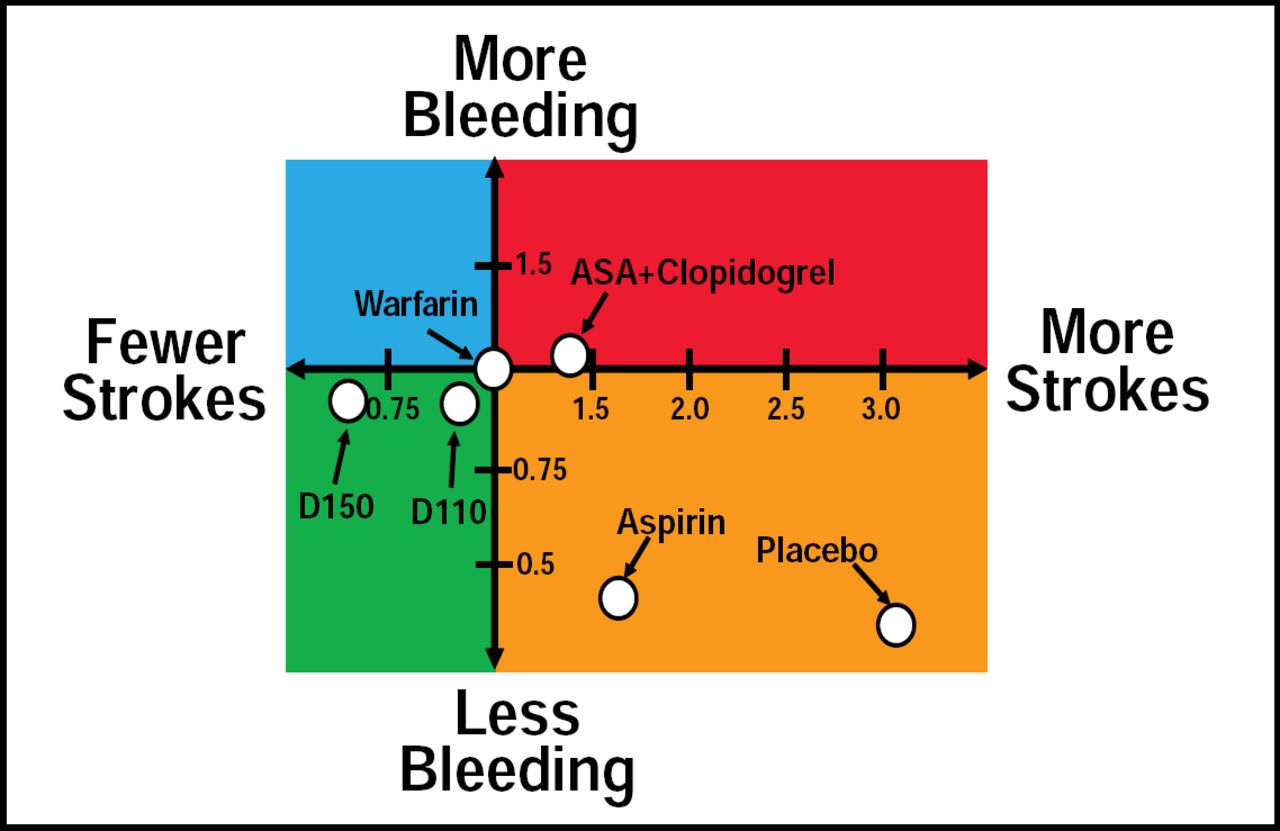
Dabigatran, a reversible oral direct thrombin inhibitor, shows promise for stroke prevention in AF. Dabigatran has a rapid onset of action and predictable and consistent anticoagulant effects without the drug-drug/drug-food interactions or cumbersome monitoring requirements that are found with warfarin. In the RE-LY study, comparing dabigatran twice daily 110 mg (D110) and dabigatran 150 mg (D150) with warfarin, D110 was associated with lower rates of major hemorrhage but similar rates of stroke and systemic embolism compared with warfarin. Meanwhile, D150 had similar rates of major hemorrhage but lower rates of stroke (including both ischemic and hemorrhagic) and systemic embolism versus warfarin [Connolly SJ et al. N Engl J Med 2009]. As the balance between stroke and bleeding prevention continues to be evaluated, the favorable results with this new agent represent the first major advance in decades (Figure 1). Of note, dabigatran is currently available in selected countries in the 110-mg formulation only. The relatively short half-life of 12 to 17 hours is an important consideration in patients for whom compliance with a twice-daily regimen is a major issue.

Antithrombotic Therapy in Perspective.
Reproduced with permission from S. La Haye, MD.
Dronedarone, a novel multichannel-blocking antiarrhythmic drug, may also be an option for stroke prevention in AF. Dronedarone has been found to reduce the incidence of hospitalization due to cardiovascular events or death in patients with AF (p<0.001) [Hohnloser SH et al. N Engl J Med 2009]. A post hoc analysis of this therapy demonstrated that dronedarone reduced the risk of stroke in this cohort, and this benefit was stronger among those with higher baseline CHADS2 scores [Connolly SJ et al. Circulation 2009]. Further evaluation of this strategy is merited to establish the effect of dronedarone on stroke prevention.
Though warfarin may be efficacious for stroke prevention in AF, it does have some shortcomings, including adherence issues, high bleeding rates, and management challenges. Novel therapies, such as combination anticoagulant regimens and newer oral anticoagulants, may provide a safe and effective alternative to warfarin treatment. Antiarrhythmic medications may also offer practical solutions to stroke risk reduction and AF management. However, it is important to balance the options carefully to ensure that the therapeutic benefit outweighs the cost.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.