

Summary
There are unique challenges of acute coronary syndrome (ACS) care in the Caribbean. When investigators examine the demographics of Caribbean patients with ACS, it is clear that patients in this region do not reflect the study populations of major ACS trials, which tend to be predominantly Caucasian.
- Myocardial Infarction
- Prevention & Screening
In a session on acute coronary syndrome (ACS), Vladimír Džavík, University of Toronto, Toronto, Ontario, Canada, described some of the unique challenges of ACS care in the Caribbean. One retrospective study showed that the annual rates of ACS hospitalization and in-hospital mortality were significantly lower in Antigua and Barbuda than in the US [Martin TC et al. West Indian Med J 2007]. The intensive care unit (ICU) admission rate in Antigua and Barbuda (0.19 to 0.73; per thousand men and women respectively) was approximately 20% of that in the US (4.1 to 1.8 per thousand), and the ICU mortality rate (0.07 to 0.04 per year) was only 10% of that reported in the US (1.0 to 0.5 per year per thousand aged 35 to 75 years). The study authors concluded that these findings illustrate a lack of access to hospital-based care for ACS patients in Antigua and Barbuda [Martin TC et al. West Indian Med J 2007].
When investigators examine the demographics of Caribbean patients with ACS, it is clear that patients in this region do not reflect the study populations of major ACS trials, which tend to be predominantly Caucasian. In one study of ACS in Trinidad and Tobago, patients were reported to primarily be of East Indian descent (62%), followed by mixed ethnicity (20%), African descent (13%), and Caucasian race (5%) [Thomas CN et al. West Indian Med J 2000]. Common risk factors in these patients included diabetes (53%), hypertension (49%), and smoking (30%). Female gender (p=0.04), in-hospital ventricular fibrillation (p=0.001), and left ventricular ejection fraction <40% (p=0.02) were independent predictors of mortality [Thomas CN et al. West Indian Med J 2000].
Other studies that have been based in the Caribbean reveal opportunities for improving several aspects of ACS care, including risk factor reduction, patient education regarding the signs and symptoms of myocardial infarction (MI), and timely use of thrombolytic therapy. For instance, in one study of ACS management in the Bahamas, the average time to presentation from the onset of symptoms of acute MI was 18 hours [Khetan et al. West Indian Med J 2000]. The majority of patients (56%) presented to a health care provider 12 hours after symptom onset. Patients were treated most commonly with oral nitrates (96%) and intravenous heparin (90%), followed by β-blockers (65%) and morphine (15%). Only 8% of patients were treated with thrombolytic agents. Cardiovascular risk factors, including hypertension (77%), obesity (62%), diabetes mellitus (35%), and smoking (25%), were common in Bahamian MI patients [Khetan et al. West Indian Med J 2000].
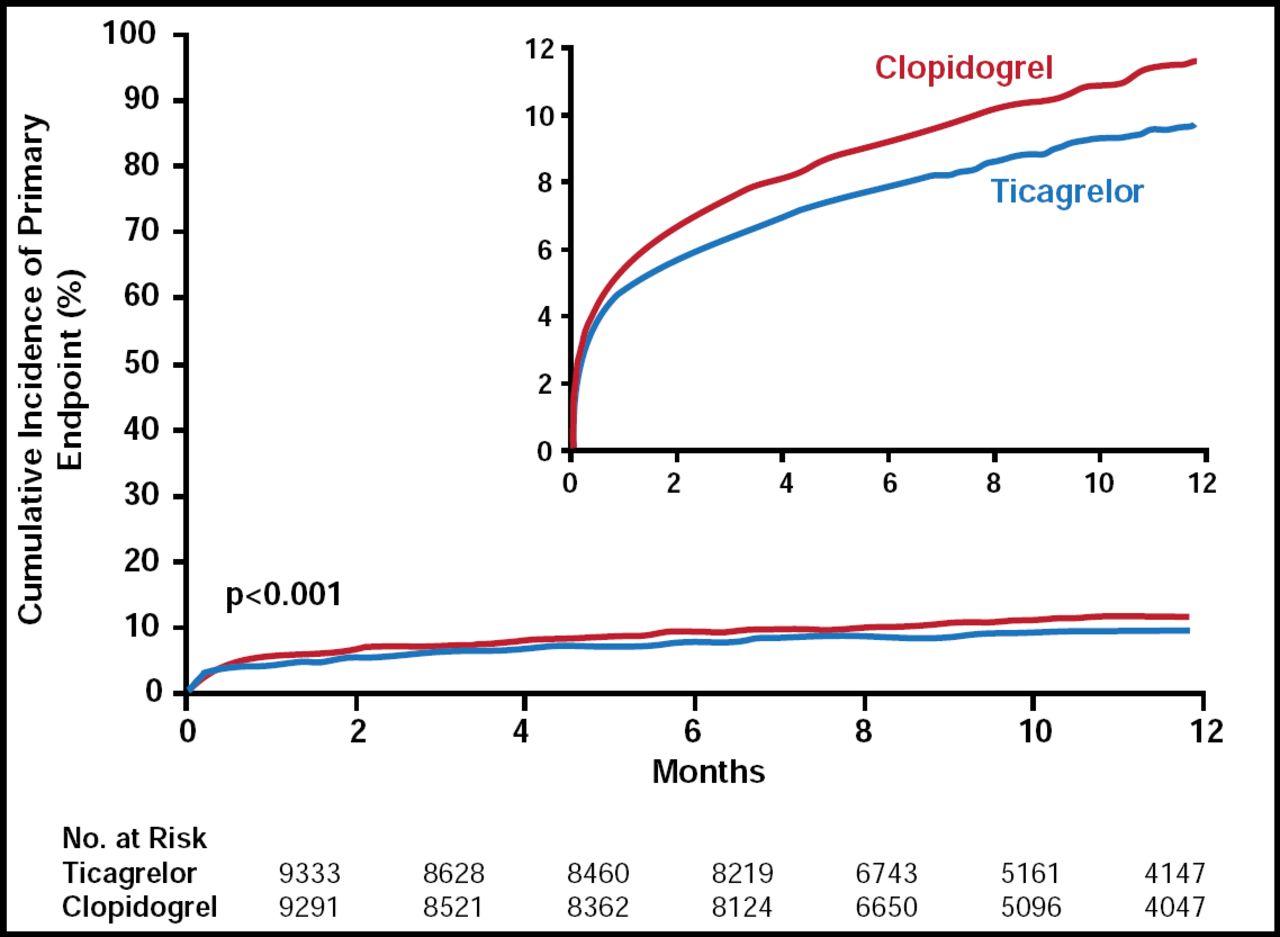
Advances in antiplatelet therapies have improved treatment options for ACS patients, particularly those who are undergoing invasive management. Refined clopidogrel regimens that include higher loading doses have reduced the risk of stent thrombosis without a significant increase in major bleeding [Mehta SR et al. ESC 2009]. Some ACS patients do not have a strong platelet inhibition response to clopidogrel and require more potent antiplatelet therapy to prevent cardiovascular (CV) events. Newer antiplatelet therapies provide even greater protection against CV events in appropriate ACS patients. Prasugrel is an irreversible oral adenosine diphosphate receptor antagonist that reduces the risk of CV death, MI, and stroke compared with clopidogrel but with an increase in the risk of major bleeding [Wiviott SD et al. New Engl J Med 2007]. Ticagrelor is an investigational oral antiplatelet agent that directly and reversibly inhibits the adenosine diphosphate receptor P2Y12. Compared with clopidogrel, ticagrelor significantly reduces the risk of CV events and death without increasing major bleeding in patients with ACS (Figure 1) [Wallentin L et al. New Engl J Med 2009].

Cumulative Kaplan-Meier Estimates of the Time to the First Adjudicated Occurrence of the Primary Efficacy Endpoint.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
Risk factors for ACS are highly prevalent among patients in the Caribbean region, and access to optimal ACS care is often limited. New research supports the use of refined ACS treatment regimens, such as an increased loading dose of clopidogrel or the use of novel antiplatelet therapies in appropriate patients. When possible, physicians should seek opportunities to apply new clinical evidence to the management of patients with ACS.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.