

Summary
Until recently, combined coronary artery disease and valvular disease treatments relied customarily on surgical intervention alone. However, traditional surgery is not without its limitations, such as significant morbidity, prolonged hospital stays, neurological complications, sternal wound infections, and high cost. New procedural options have emerged, offering less invasive solutions to cardiac issues with fewer treatment obstacles. Hybrid procedures create a more collaborative treatment environment and may provide improved outcomes and long-term survival benefits compared with traditional surgery.
- Coronary Artery Disease
- Valvular Disease
- Interventional Techniques & Devices
Until recently, combined coronary artery disease (CAD) and valvular disease treatments relied customarily on surgical intervention alone. However, traditional surgery is not without its limitations, such as significant morbidity, prolonged hospital stays, neurological complications, sternal wound infections, and high cost. New procedural options have emerged, offering less invasive solutions to cardiac issues with fewer treatment obstacles. Hybrid procedures create a more collaborative treatment environment and may provide improved outcomes and long-term survival benefits compared with traditional surgery. Kevin Coy, MD, FACP, Jackson International, Miami, Florida, USA, discussed some of these promising models and how they may benefit regions, such as the Caribbean.
Hybrid procedures entail collaborations between surgeons, interventional cardiologists, and other specialists in order to foster a multidisciplinary approach to treatment, with a goal of developing less invasive treatment protocols when possible. Combined strategies and diagnostic modalities may introduce innovative treatment methods and considerations in a previously limited area of medicine. In order to encourage this collaborative relationship, training programs may be incorporated into current clinical models.
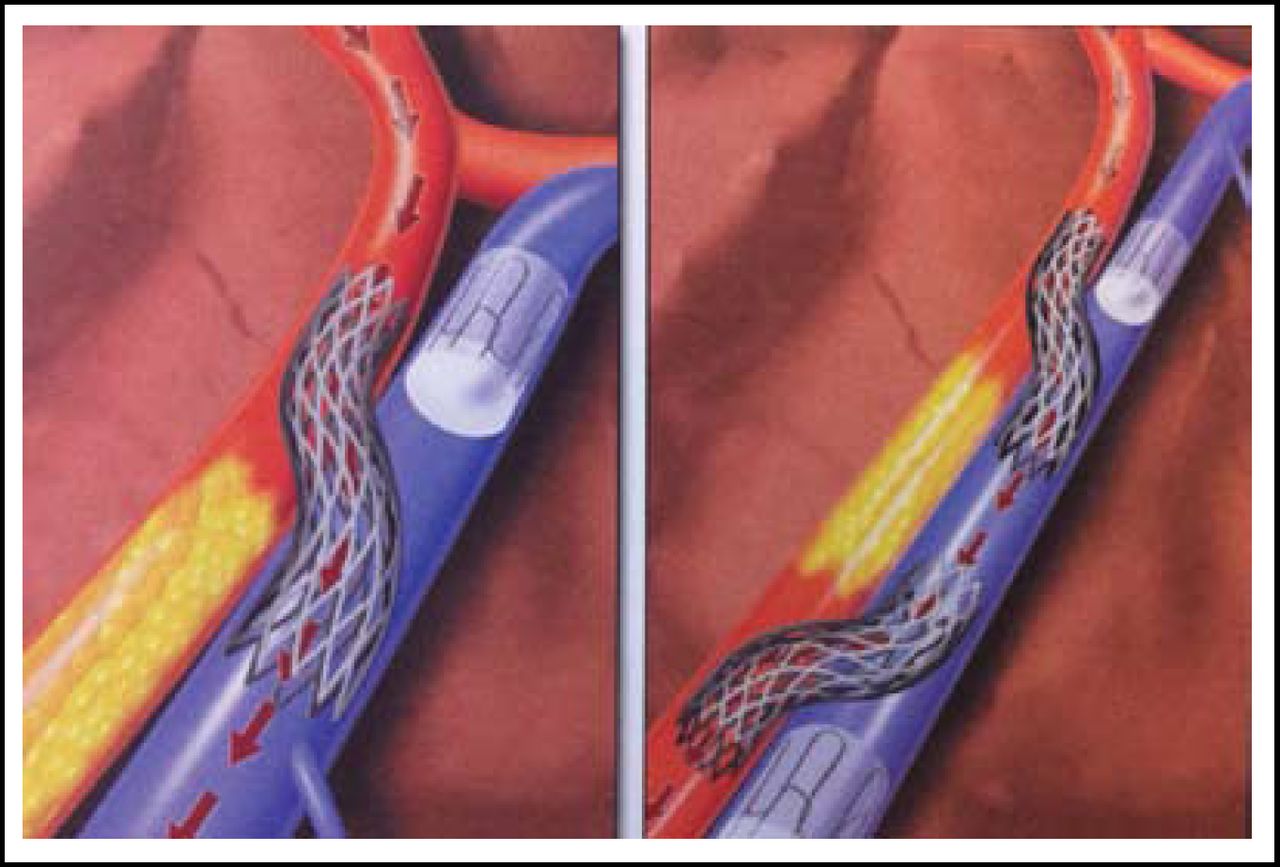
There are numerous percutaneous procedures on the horizon that, while not yet widely available, provide hope for the future. Among these less invasive strategies are percutaneous valve (aortic and mitral repair) and novel percutaneous in situ coronary artery bypass procedures (Figure 1). The percutaneous aortic valve employs the transapical approach and utilizes bovine pericardium. The self-expanding nitinol frame mimics the robust surgical valve design, while the support frame facilitates intuitive and accurate deployment of the valve. Further evaluation of these options is required to determine their durability and associated long-term outcomes.

Percutaneous in situ Coronary Venous Arterialization (left) and Catheter-Based Coronary Bypass (right).
Reproduced with permission from K. Coy, MD.
Coronary angiography is often used in the interventional setting and is a helpful tool for preoperative assessment prior to noncoronary cardiac surgeries. This diagnostic procedure may be a suitable augmentation to hybrid procedures that stem from multidisciplinary collaborations. Alan Smith, MD, Queen Elizabeth Hospital, Barbados, West Indies, evaluated the use of coronary angiography at his institution in patients who were referred for noncoronary cardiac surgery. The goal of this retrospective study was to assess the utility of coronary angiography according to current American Heart Association/American College of Cardiology 2006 guidelines for the management of valvular heart disease (Class I, IIa, and III) and to determine the accuracy of the age-related recommendations for routine coronary angiography for noncoronary cardiac surgery in this cohort.
This retrospective review included 111 cases who were referred for noncardiac surgery (age range 40 to 77 years; median age 56 years). Twenty-five patients who underwent coronary angiography were aged <50 years. Sixteen patients had CAD, 7 of whom did not require revascularization; all were hypertensive. Nine patients had coronary bypass grafting. Pathology data are listed in Table 1.
Pathology Data.
Based on data from this specific population, Dr. Smith and colleagues concluded that for patients without CAD risk factors who present for noncoronary cardiac surgery, the recommended age for coronary angiography should be raised from 40 to 50 years. Additionally, when CAD risk factors are present, coronary angiography is suitable prior to noncoronary cardiac surgery for patients of all ages. Further statistical analysis and more specific risk parameters should be investigated in a prospective study that includes a broader cohort prior to modifying clinical perspectives on coronary angiography. This evaluation was based on limited data in a very specific cohort.
Clinicians are beginning to modify their approaches to CAD and valvular disease as new technologies and procedures emerge. Avoiding unnecessarily invasive procedures and encouraging alternative methods have become priorities. However, there is still progress to be made prior to the implementation of many of these innovative strategies. Incorporating multidisciplinary approaches and reliable diagnostic modalities with novel procedures may allow for less invasive solutions to cardiac problems in the future.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.