

Summary
Exercise electrocardiogram (ECG) testing has a low predictive value for significant coronary artery disease in Caribbean patients. Additionally, electrophysiology studies and radiofrequency ablation therapy have become the standard of care for the chronic management of many cardiac arrhythmias. This article discusses these imaging modalities from a Caribbean perspective.
- Interventional Techniques & Devices
- Cardiac Imaging Techniques
- Imaging Modalities
- Coronary Artery Disease
Exercise electrocardiogram (ECG) testing has a low predictive value for significant coronary artery disease (CAD) in Caribbean patients, according to new research from the University Hospital of the West Indies (UHWI). Taleya Girvan, BSc, MBBS, UHWI, Mona, Jamaica, described findings from 3 years of institutional experience with exercise stress testing.
Physicians at UHWI routinely perform ECG stress tests to determine whether patients with chest pain or heart failure symptoms have significant CAD and, therefore, need additional evaluation with coronary angiography. According to previous studies, ST-segment depression on stress testing has a high specificity for CAD (83% to 97%) and variable sensitivity for 1-vessel disease (25% to 60%), 2-vessel disease (91%), and 3-vessel disease (73% to 100%). However, given that these studies were performed in predominantly male and Caucasian populations, it is unclear whether the sensitivity and specificity findings also apply to different patient populations.
In this retrospective study, Dr. Girvan and colleagues reviewed data from all patients who underwent exercise stress testing at UHWI from August 2006 through August 2009. Patients with positive stress test results were categorized according to their probability of having CAD (high, intermediate, or inconclusive). Patients with negative stress tests results were defined as having a low probability of CAD. The investigators also examined angiographic results in the subgroup of patients with positive stress test results who underwent coronary angiography. Angiographic results were categorized as normal, CAD with significant stenosis, or CAD with nonsignificant stenosis.
A total of 997 exercise stress tests were performed during the 3-year data collection period. Of them, 256 were positive and 741 were negative. Within the subgroup of patients with positive ECG results, 81 patients went on to receive 83 angiograms. The angiography group included 48 women (59%) and 33 men (41%), with a mean age among all patients of 59.2 years.
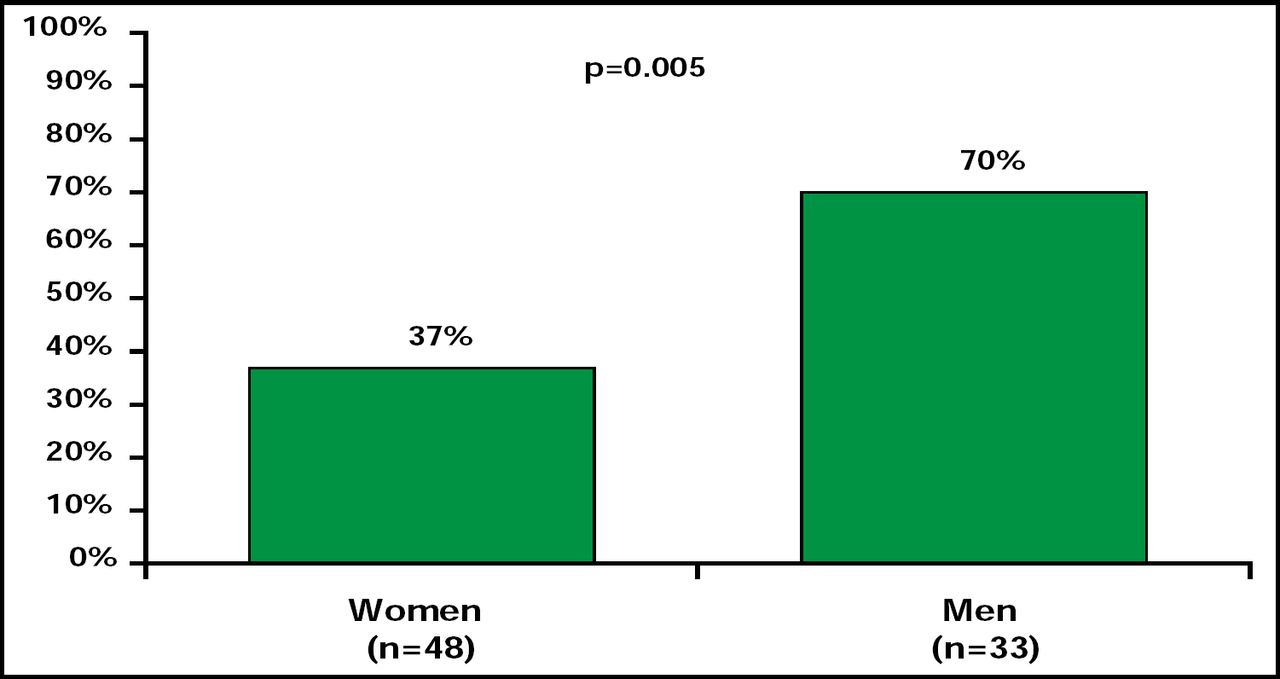
At angiography, 67 patients (70%) were found to have CAD, but only 38 patients (47%) had CAD with significant stenosis. The remaining patients had CAD with nonsignificant stenosis (36%) or normal vessels (17%). Compared with female patients, male patients were significantly more likely to be diagnosed with significant stenosis (37% vs 70%; p=0.005; Figure 1).

Prevalence of CAD with Significant Stenosis Among Patients with Positive Exercise Stress Test Results.
Reproduced with permission from T. Girvan, BSc, MBBS.
Despite the low predictive value that was calculated here (47%), the true utility of exercise stress testing in evaluating patients for the presence of significant CAD remains unclear, Dr. Girvan said. This small retrospective study was limited by the low number of patients with positive stress test results who underwent angiography, a short study period, and missing results for many patients. Future studies should evaluate additional patient data, including history of diabetes or hypertension; smoking history; family history of cardiovascular disease; cholesterol and high-sensitivity C-reactive protein levels; duration of symptoms; chest pain etiology (typical vs atypical); and history of stable angina, unstable angina, myocardial infarction, or hospital admission for acute coronary syndrome. With this information, future studies may able to determine definitively whether ECG stress testing is a useful tool for CAD screening in the Caribbean patient population.
Cardiac Ablation Therapy: The Trinidad and Tobago Experience
Electrophysiology (EP) studies and radiofrequency (RF) ablation therapy have become the standard of care for the chronic management of many cardiac arrhythmias. In Trinidad and Tobago, these procedures were traditionally performed by electrophysiologists from visiting Johns Hopkins Medicine International (JHMI) and other international medical programs. In June 2009, Trinidad gained its first resident electrophysiologist to provide this specialized care for patients with arrhythmias. Lana Boodhoo, MD, Eastbourne General Hospital, Eastbourne, UK, described findings from a survey of cardiac EP procedures that were performed in Trinidad and Tobago.
Cardiologists in Trinidad and Tobago face several challenges in the delivery of cardiac care. Physicians have access to three cardiac catheterization laboratories and surgical support, but few options for cardiac ablation therapy. Treatment centers lack specialized ablation equipment, such as electroanatomical mapping systems, intracardiac ultrasound, equipment for internal cardioversion, and must lease equipment and technical support as needed from other countries. Centers do have access to noninvasive equipment, including Holter monitors, echocardiography equipment, event monitors, cardiac computed tomography (CT), and positron emission tomography (PET) imaging.
Other challenges in Trinidad include a limited choice of antiarrhythmic drugs, no local access to genetic testing, and no software for electrocardiography signal averaging. With these limitations, physicians do not perform EP procedures on patients with atypical atrial flutters, atrial fibrillation, or ventricular tachycardia (VT). Currently, catheter ablation is available only for patients with atrioventricular nodal reentrant tachycardia (AVNRT), atrioventricular reentrant tachycardia (AVRT), atrial tachycardia, atrial flutter, atrioventricular (AV) nodal ablation, or right ventricular outflow tract (RVOT) VT.
Between July 2009 and July 2010, 63 patients were treated with 67 ablation procedures by the resident electrophysiologist and visiting JHMI faculty. Steps in the ablation procedure included light sedation, induction and mapping of the arrhythmia, and postablation arrhythmia induction. The mean patient age was 46 years (range, 9 to 89 years), and patients had arrhythmia for a mean duration of 4 years prior to their procedure. The most commonly used antiarrhythmic drugs were calcium channel blockers (32%) and amiodarone (31%), followed by β-blockers (24%) and flecainide (3%).
In all procedures that involved AVNRT (n=22), atrial flutter (n=11), atrial tachycardia (n=5), and AV nodal ablation (n=4), full ablation was achieved. Cardiac ablation was also successful in 10 of 12 (83%) AVRT procedures and 1 of 2 (50%) RVOT VT procedures. Only 1 complication (1%) was reported, and no recurrences were observed.
As demonstrated in Trinidad, simple interventional EP procedures can be performed safely and effectively in local cardiology centers. While resources for complex ablation procedures are lacking, simple ablation is an option that is underutilized, in part due to poor referral rates from community centers. Dr. Boodhoo found that some community physicians are relying on the inappropriate use of amiodarone to manage supraventricular tachycardia.
Dr. Boodhoo offered several recommendations to improve access to EP procedures in Trinidad and Tobago. For instance, the cardiology community should develop a national cardiology framework with specific guidelines for the management of arrhythmia. Medical organizations should work toward implementing arrhythmia guidelines and monitor compliance to guideline-recommended care across community cardiology centers. Trinidad and Tobago should also commit to investments in infrastructure, equipment, and personnel. Together, these efforts will improve outcomes for patients with a range of cardiac arrhythmias, Dr. Boodhoo concluded.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.