

Summary
Cardiovascular disease, now the leading cause of death both in the United States and worldwide, is responsible for approximately 16.7 million deaths per year. In the past decade, widespread interventions, such as aspirin and statin therapy and smoking cessation, have contributed to a 29% reduction in the risk of cardiovascular mortality [Lloyd-Jones D et al. Circulation 2010]. However, the increased prevalence of obesity, diabetes, and sedentary lifestyle has outpaced other benefits, leading to an increased risk for coronary heart disease (and myocardial infarction. This article discusses emerging trends in intensive lipid management.
- Lipid Disorders
Cardiovascular disease (CVD), now the leading cause of death both in the US and worldwide, is responsible for approximately 16.7 million deaths per year. In the past decade, widespread interventions, such as aspirin and statin therapy and smoking cessation, have contributed to a 29% reduction in the risk of cardiovascular (CV) mortality [Lloyd-Jones D et al. Circulation 2010]. However, the increased prevalence of obesity, diabetes, and sedentary lifestyle has outpaced other benefits, leading to an increased risk for coronary heart disease (CHD) and myocardial infarction (MI). In this session, Robert P. Giugliano, MD, SM, Brigham and Women's Hospital, Boston, Massachusetts, USA, discussed emerging trends in intensive lipid management.
Traditional risk factors, including high cholesterol, smoking, hypertension, diabetes, and obesity, explain the majority of the risk for CV events. Accordingly, therapeutic lifestyle changes form the basis of modern treatment strategies. Patients with a higher baseline risk also need pharmacological therapy for effective risk factor reduction. Yet, for many patients, efforts toward CV risk reduction are insufficient to prevent major cardiac events. In a review of 231,986 hospitalizations for an acute coronary event, only 21% of all patients were taking lipid-lowering medications prior to admission. Among those with a prior history of coronary artery disease (CAD), only 29% had been taking lipid-lowering therapy at the time of their acute coronary event [Sachdeva A et al. Am Heart J 2009].
Aggressive Lipid Lowering with Therapy
To date, statins are the best studied options for lipid-lowering therapy. Statin monotherapy can reduce low-density lipoprotein cholesterol (LDL-C) levels by 38% to 49%, while statin-based combination regimens can lower LDL-C by 62% [Hochhlozer W, Giugliano R. Ther Adv Cardiovasc Dis 2010]. How much LDL-C reduction is enough? Data modeling suggests that the incidence of CV events can be reduced to almost zero with LDL-C targets of <60 mg/dL for primary prevention and <30 mg/dL for secondary prevention [Hochhlozer W, Giugliano R. Ther Adv Cardiovasc Dis 2010]. Achieving these goals will require much more potent lipid-lowering regimens. Aggressive lipid-lowering therapy can be particularly beneficial among patients with high pretreatment LDL-C values [Giraldez RR et al. J Am Coll Cardiol 2008].
For patients who fail to reach LDL-C targets with statin therapy alone, statin-based combination therapy may provide additional incremental benefits in CV risk reduction. In the Ezetimibe and Simvastatin in Dyslipidemia of Diabetes (ESD) trial, the addition of ezetimibe to simvastatin provided significantly greater LDL-C reduction than simvastatin alone in patients with diabetes and dyslipidemia (Figure 1) [Ruggenenti P et al. Diabetes Care 2008]. Various statin-based combination therapies are also being studied in patients with ACS, CAD, kidney failure, and established vascular disease (Table 1).
Ongoing Trials of Statin-Based Combination Therapy.

Improved LDL Reduction with Combination Ezetimibe/Simvastatin.
Reproduced with permission from R. Giugliano, MD, SM.
Non-LDL-C Treatment Targets
According to data from the Framingham Heart Study, high-density lipoprotein cholesterol (HDL-C) is a predictor of risk for CHD, even among patients with low LDL-C levels [Gordon T et al. Am J Med 1977]. Non-HDL lipoproteins, including very low-density lipoprotein cholesterol (VLDL-C), are also atherogenic [Grundy SM et al. Circulation 2004]. Current guidelines from the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III) recommend lowering elevated HDL and non-LDL cholesterol levels as part of a comprehensive strategy to reduce the risks that are associated with a proatherogenic lipid profile [NCEP. JAMA 2001]. In patients with triglyceride (TG) levels ≥200 mg/dL, LDL-C reduction remains the primary goal of treatment. In these patients, non-HDL-C is a secondary target of treatment, with a goal of 30 mg/dL higher than the LDL-C goal. In contrast, when TG levels are >500 mg/dL, non-HDL-C should be the primary target of treatment [NCEP. JAMA 2001].
Several drug classes appear to provide modest increases in HDL-C levels, including niacin (15% to 35%), fibrates (10% to 15%), estrogens (10% to 15%), and statins (5% to 10%) [Belacazar LM et al. Progr Cardiovasc Dis 1998]. Investigational agents that are designed specifically to increase HDL-C levels, such as cholesteryl ester transfer protein (CETP) inhibitors, have not yet demonstrated clinical efficacy to date. In the Investigation of Lipid Level Management to Understand its Impact in Atherosclerotic Events (ILLUMINATE) trial, treatment with the CETP inhibitor torcetrapib, when added to atorvastatin, increased HDL-C levels by 72% at 12 months. However, the addition of torcetrapib to statin therapy increased the risk of CV events by 25% (p=0.001) and increased all-cause mortality by 58% (p=0.006) [Barter PJ et al. N Eng J Med 2007]. Studies of two other investigational CETP inhibitors, dalcetrapib and anacetrapib, are currently underway.
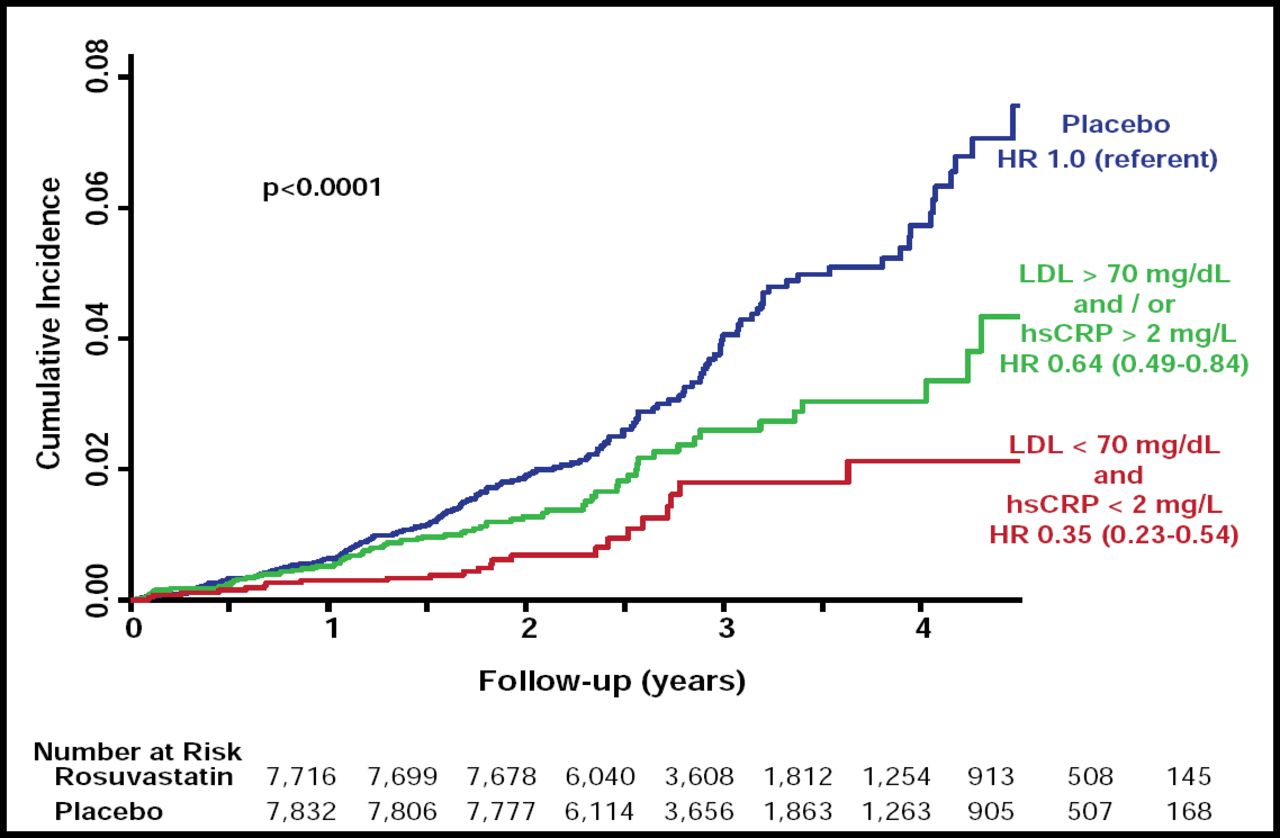
Aggressive statin therapy may provide important clinical benefits that are independent of LDL-C reduction. Mega and colleagues recently showed that high-dose statin therapy, before elective percutaneous coronary intervention (PCI), prevents myocardial damage and reduces the risk of postprocedure MI [Mega S et al. Crit Path Cardiol 2010]. In the Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER), reduction of high-sensitivity C-reactive protein (hsCRP) was an important indicator of treatment success. Rosuvastatin-treated patients who achieved low LDL-C levels (<70 mg) and low hsCRP levels (<2 mg/L) had the best clinical outcomes (Figure 2) [Ridker PM et al. N Eng J Med 2009]. These findings suggest the importance of targeting additional markers of CV risk in primary and secondary prevention. To close the major treatment gap toward reduced CV morbidity and mortality, future management of dyslipidemia promises to include more potent LDL-lowering regimens, as well as non-LDL targets, such as HDL-C, non-HDL-C, and CRP.

JUPITER: Incidence of CV Events According to Whether Reductions in Both LDL-C and hsCRP Are Achieved.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.