

Summary
The frequency of open heart surgery procedures that are performed in Trinidad and Tobago has increased since procedures began being performed at the Eric Williams Medical Science Complex in 1993, and by 2006, over 200 cases per year were being performed nationally. This increase in cardiac surgery within the region poses additional clinical challenges that are related to the use of blood products, such as adding to the burden of already limited blood bank resources, the high cost of blood product screening, and the risks of transfusion-related diseases and potential bleeding complications.
- Interventional Techniques & Devices Clinical Trials
The frequency of open heart surgery procedures that are performed in Trinidad and Tobago has increased since procedures began being performed at the Eric Williams Medical Science Complex in 1993, and by 2006, over 200 cases per year were being performed nationally. This increase in cardiac surgery within the region poses additional clinical challenges that are related to the use of blood products, such as adding to the burden of already limited blood bank resources, the high cost of blood product screening, and the risks of transfusion-related diseases and potential bleeding complications. In this region, the issue of short preoperative periods for patient optimization compounds the problem. “The challenge was in finding ways not to just increase supply but also to minimize the utilization of blood products,” explained Ronald Henry, MD, The Doctors Inn Research Group, Trinidad and Tobago.
In an effort to resolve the mounting problem of blood product scarcity and overutilization of resources, Dr. Henry and colleagues developed strategic initiatives that were evaluated at the Port-of-Spain General Hospital. The first initiative focused on preoperative preparation, including holding aspirin or Plavix prior to surgery to minimize blood loss, securing the appropriate number of blood units, and implementing a standard protocol to optimize hemoglobin (Hb) levels prior to surgery, with a target Hb of >15.0 g/dL (Table 1).
Protocol to Optimize Hb Levels Prior to Cardiac Surgery (Target Hb >15.0 g/dL).
Another strategy that Dr. Henry and colleagues employed in this program involved hospital laboratory cooperation. Hospital laboratories were asked to consistently provide proper and dedicated refrigeration facilities to allow for a protocol-based return of unused blood, and crossmatching of blood products was part of a pooled analysis that involved multiple potential recipients. Intraoperative management approaches included the use of “Cell Saver” devices, which allow for the reinfusion of blood at the end of the operative process, limiting unnecessary waste, and the prophylactic use of intravenous tranexamic acid to reduce postoperative bleeding. Postoperative protocols were also employed that consisted of stringent indications for transfusion and restriction of utilization to essential candidates.
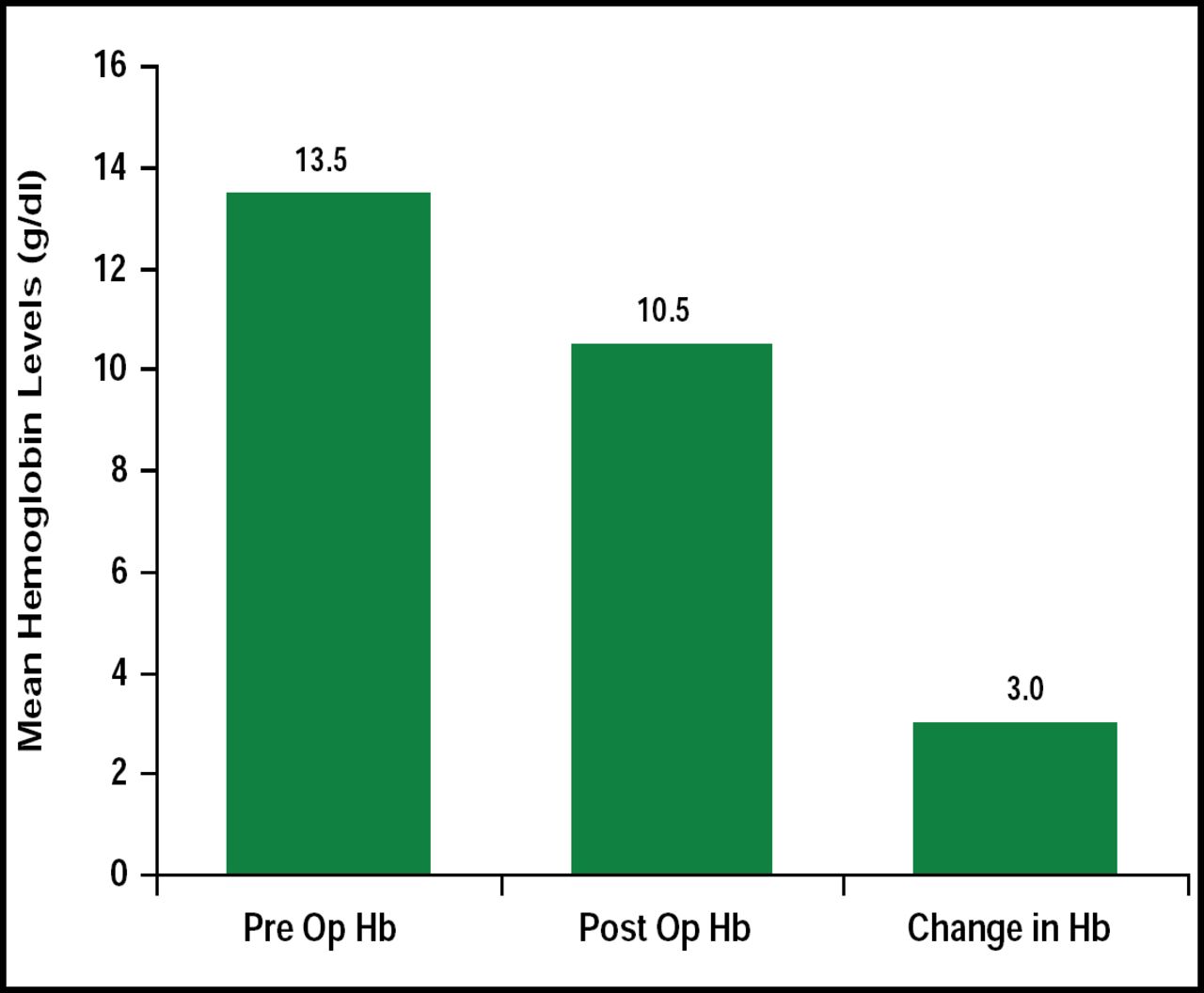
From September 2006 to November 2009, a total of 227 cardiac surgery procedures (the majority of which was bypass or valve procedures) were evaluated. There were 5 deaths, and the in-hospital mortality rate was 2.2%. Almost all patients who underwent cardiac surgery required preoperative iron therapy, but postoperative Hb ranges were favorable, with 40% of patients in the >11 g/dL range (Figure 1). Thirty-six percent of patients received 200–300 mL of blood that was returned to them due to cell saver therapy, which negated the need for transfusion in this cohort. Most importantly, this study marks the first time that blood was ever returned to the blood bank, despite the previous protocols that were in place, concluded Dr. Henry.

Preoperative and Postoperative Mean Hb Levels (g/dL).
Reproduced with permission from R. Henry, MD.
This evaluation demonstrated the benefit of preoperative optimization of hemoglobin in patients who were undergoing cardiac surgery in a region where blood product resources are a concern. The use of “cell saver” approaches may also reduce the need for transfusion in many patients, thus lowering transfusion-related complication rates. Collaboration with blood banks and specific protocols, as seen in this study, may also optimize blood product utilization. The development of standardized protocols to manage this medical need is necessary in order to reduce the burden that is associated with blood product scarcity in this and other regions that are faced with this same clinical challenge.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.