

Summary
Traumatic aortic transection (TAT) is a rare but often fatal condition, with ∼70% of these events caused by blunt motor vehicle trauma (it is the second most common cause of motor vehicle accident mortality) [Michetti et al. J Trauma 2006]. While the majority of patients dies at the scene of the accident, the prognosis for those who initially survive remains dire, with 90% of deaths occurring within 4 months post-aortic transection. This article presents management strategies for TAT.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
Traumatic aortic transection (TAT) is a rare but often fatal condition, with ∼70% of these events caused by blunt motor vehicle trauma (it is the second most common cause of motor vehicle accident mortality [MVA]) [Michetti et al. J Trauma 2006]. While the majority of patients dies at the scene of the accident, the prognosis for those who initially survive remains dire, with 90% of deaths occurring within 4 months post-aortic transection. Joseph L. Blidgen, MD, MBBS, University Hospital of the West Indies (UHWI), Kingston, Jamaica, discussed management strategies for TAT, related to 5 cases that were seen at his institution between April 2006 and February 2010.
Diagnostic imaging modalities, such as chest x-ray, angiography, and computed tomography (CT) angiography, which is the current gold standard, are the first step in identifying TAT, particularly among patients who have been involved in a MVA. Further management of TAT may involve adjunctive medical therapy (ie, antihypertensive or β-blocker treatment), open repair (ie, clamp and sew or shunt bypasses), endovascular stenting, or a combination of these methods. Dr. Blidgen cautioned that life-threatening injuries (ie, severe head and abdominal injuries) should be given priority over TAT when present.
Dr. Blidgen and colleagues followed 5 cases of TAT that resulted from MVAs at UWHI. All 5 patients were unrestrained during the MVA, 3 were back seat passengers and 2 were front seat passengers (age range was 15 to 29 years). One patient was diagnosed intraoperatively and referred 4 hours post-MVA once control of intraabdominal bleeding was achieved, 3 were referred 12 hours post-MVA, and 1 was referred 2 weeks post-MVA. Excluding the 15-year-old female who was diagnosed intraoperatively, TAT was diagnosed using chest x-ray and contrast CT scan.
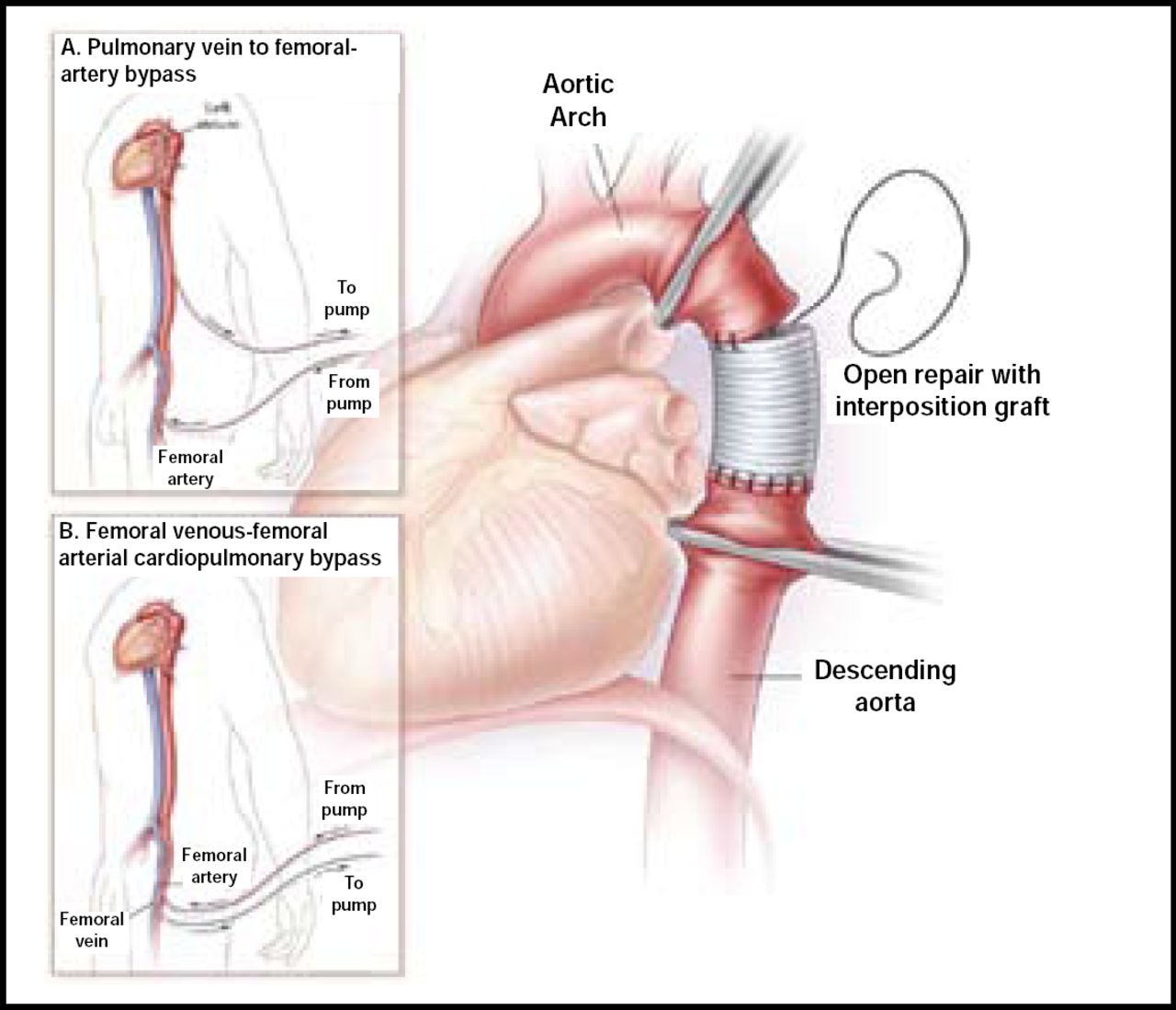
Three patients underwent surgical repair with cardiopulmonary bypass, 1 had left thoracotomy and clamp and sew technique without cardiopulmonary bypass, and 1 patient refused surgical intervention (Figure 1). Of the 4 patients who underwent surgical intervention, 2 had interposition graft placement and 2 had direct repair. One patient had subsequent paraplegia, but there were no reported deaths.

Repair Techniques.
Reproduced with permission from J. Blidgen, MD.
Endovascular repair is another option for TAT management. It is less invasive than open repair; avoids thoracotomy, single lung ventilation, systemic heparinization, and other potential complications; and can be performed using localized anesthesia. However, it is a relatively new technique; so the long-term prognosis that is associated with this procedure is unclear. Additionally, it may introduce ischemia in other regions, such as the arm or vertebral artery. While this may be a more viable option in the future, these concerns, as well as cost constraints, make endovascular repair less practical at present. Dr. Blidgen concluded that the standard open surgical approach to TAT remains the preferred strategy for the treatment of this complex condition.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.