

Summary
This article discusses findings from this phase III, multicenter, parallel-group, double-blind, randomized placebo-and active-controlled trial [NCT00696241]. The purpose of this study was to compare the BP lowering effects of azilsartan medoxomil with olmesartan medoxomil and placebo over a period of 6 weeks in patients with primary hypertension.
- Hypertensive Disease Clinical Trials
In a recent study comparing azilsartan medoxomil (AZL-M) with olmesartan medoxomil (OLM-M) and placebo, AZL-M therapy was found to be safe and effective in patients with primary hypertension. Angiotensin receptor blockers (ARB) such as OLM-M are thought to be better tolerated than other classes of antihypertensives. However, many patients continue to experience inadequate blood pressure (BP) control despite medical therapy. Therefore, more therapeutic options are being investigated in the hopes of providing more reliable BP control. OLM-M was chosen as a comparative ARB due to its similarity to AZL-M with regards to its mechanism of action.
George L. Bakris, MD, University of Chicago Medical Center, Chicago, Illinois, USA, presented findings from this phase III, multicenter, parallel-group, double-blind, randomized placebo-and active-controlled trial (NCT00696241). The purpose of this study was to compare the BP lowering effects of AZL-M with OLM-M and placebo over a period of 6 weeks in patients with primary hypertension.
A total of 1275 patients were randomized to receive AZL-M 20 mg daily (n=283), AZL-M 40 mg daily (n=283), AZL-M 80 mg daily (n=285), OLM-M 40 mg daily (n=282) or placebo (n=142) and BP was evaluated using ambulatory BP monitoring (ABPM) and clinic BP measurement. Patients with trough sitting clinic diastolic BP >114 mm Hg, history of a major cardiovascular event, secondary hypertension, hyperkalemia, renal artery stenosis, or Type 1/poorly controlled diabetes were excluded from participation in the study. The groups were well-matched at baseline with regards to demographics and BP readings.
The primary endpoint was change in 24-hour mean systolic BP (SBP) from baseline to Week 6, as determined by ABPM. The secondary efficacy endpoints included change from baseline to Week 6 in trough sitting clinic SBP, 24-hour mean sitting diastolic BP (DBP) according to ABPM, and other ABPM parameters, such as mean trough BP at 22 to 24 hours post-dosing. Secondary safety endpoints included adverse events and laboratory data.
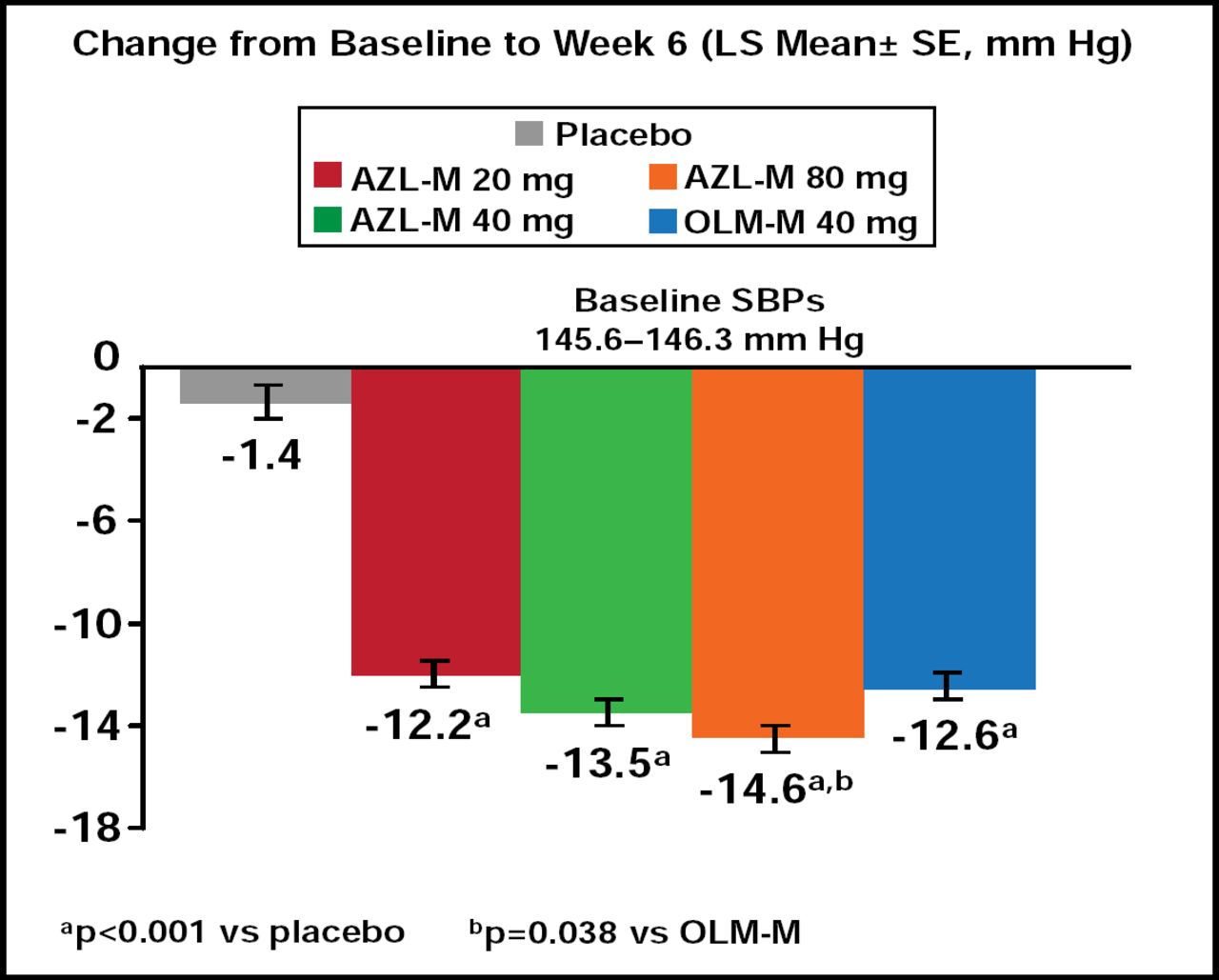
Treatment with all doses of AZL-M resulted in significantly lower 24-hour mean SBP compared with placebo at Week 6 (p<0.001 for all doses). This was also the case with 24-hour mean DBP in AZL-M patients versus placebo (0<0.001 for all doses). Patients taking AZL-M 80 mg had significantly reduced 24-hour mean SBP compared with OLM-M 40 mg (p=0.038; Figure 1). The AZL-M 80 mg group also demonstrated significant improvement in trough sitting clinic SBP and DBP at Week 6 compared with OLM-M 40 mg (p=0.043 and p=0.044, respectively).

24-Hour Mean SBP by ABPM.
Serious adverse events occurred in 2.1% of patients in the placebo group, 2.8% in the AZL-M 20 mg group, 0.4% in the AZL-M 80 mg group, and 0.7% in the OLM-M group. No serious adverse events were reported in the AZL-M 40 mg group. A total of 30 patients discontinued treatment due to adverse events (6 in placebo, 11 in AZL-M 20 mg, 3 in AZL-M 40 mg, 6 in AZL-M 80 mg, and 4 in OLM-M 40 mg group). One death did occur in the AZL-M 20 mg group. Overall, the safety profiles of all AZL-M doses were similar to that of OLM-M and placebo.
These findings demonstrate that AZL-M is safe and effective for the treatment of primary hypertension. It is important to note that AZL-M is not currently licensed for the treatment hypertension. However, these results are quite promising and warrant further investigation.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.