

Summary
Every 30 seconds, a lower limb is lost due to complications of diabetes www.diabeticfootonline.com]. This article discusses management strategies for the treatment of the diabetic foot wound.
- Diabetes Mellitus
David G. Armstrong, DPM, MD, PhD, University of Arizona College of Medicine, Tucson, AZ, presented the 2010 Roger Pecoraro Lecture at the American Diabetes Association 70th Annual Scientific Sessions, where he discussed management strategies for the treatment of the diabetic foot wound. Every 30 seconds, a lower limb is lost due to complications of diabetes [www.diabeticfootonline.com]. According to the Nord-Trondelag Health Study, foot ulcer history is associated with a 38% increased risk of death among diabetics after adjusting for lifestyle and demographic factors [Iverson MM et al. Scandinavian J Public Health 2008].
Dr. Armstrong recommends the team approach to diabetic foot wound management in order to reduce the incidence of amputation. In a study that evaluated 1708 procedures over a period of 32 months, patients who received the team approach to treatment were 61.0% less likely to undergo amputation versus 28.9% in the control group (p<0.0001) [Armstrong DG et al. ADA 2010]. An effective amputation prevention team should include the ability to perform certain tasks, such as site-appropriate culture techniques, vascular assessment and revascularization, neurological evaluation, wound assessment and infection staging/grading, site-specific bedside and intraoperative incision and debridement, culture- and patient-appropriate antibiotic therapy implementation, and postoperative monitoring with a focus on reulceration and infection risk reduction [Fitzgerald et al. EPlasty 2009; Armstrong DG et al. JVS 2010].
There are also many advances being made in the area of wound care that may optimize the management of diabetic foot ulcers. Among them is vacuum-assisted closure (VAC) therapy. This therapy provides several healing advantages, such as promotion of flap and graft survival, removal of interstitial fluid and infectious material, and uniform wound closure through the use of negative pressure [Saxena et al. Plast Reconstr Surg 2004]. VAC therapy resulted in fewer surgical procedures and dressing changes compared with standard moist wound therapy (p<0.0001 for both) [Apelqvist J et al. Am J Surg 2008].
Receptor activator of nuclear factor kappa B ligand (RANK-L), osteoprotegerin (OPG), and intranasal calcitonin may also facilitate healing in diabetic foot ulcers. RANK-L and OPG play a key role in bone remodeling and resorption. Dysregulation of RANK-L or OPG may result in bone loss. Upregulation of RANK-L may occur in the presence of peripheral neuropathies. Intranasal calcitonin may reduce bone turnover, a product of the RANK-L/OPG system, by inhibiting RANK-L. Unlike bisphosphonates, intranasal calcitonin may be used in patients with renal insufficiency [Bern et al. Diabetes Care 2004; Bern et al. Diabetologia 2006].
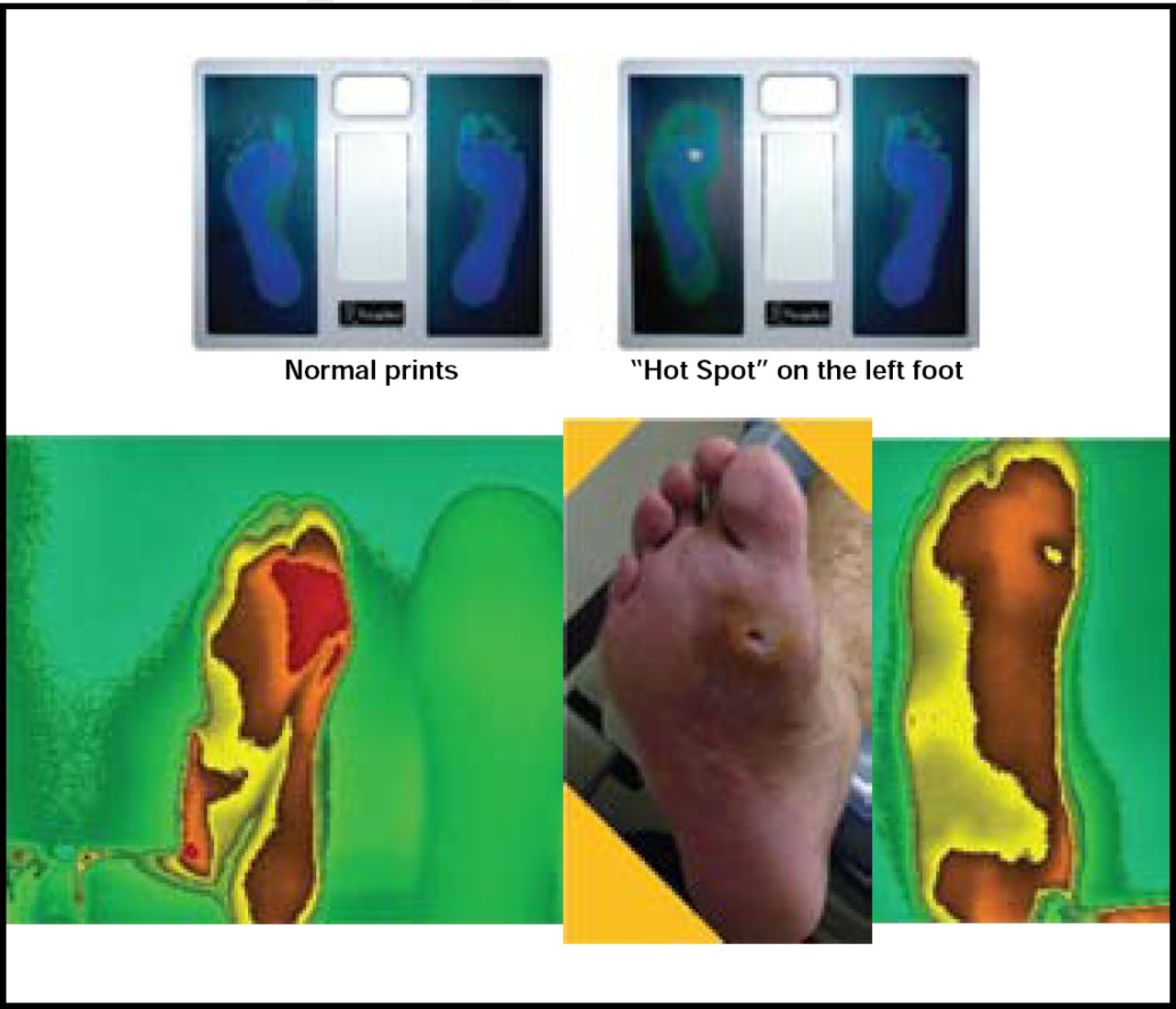
Preventing a recurrence remains a priority in diabetic foot ulcer management. Cumulative risk for ulceration by foot risk category may be one way of predicting recurrence. The risk groups range from 0 to 3 based on history and the presence of neuropathy or peripheral vascular disease (0=no neuropathy, no PVD; 1=neuropathy+/− deformity; 2=PVD +/− neuropathy; 3=history of pathology). Skin temperatures may provide important predictive data and indicate impending ulcerations. High temperature gradients between feet may predict the onset of neuropathic ulceration, and regular monitoring of bilateral foot temperatures may allow for early intervention and prevention (Figure 1) [Armstrong DG et al. Phys Ther 1997; Armstrong DG et al. Am J Med 2008; Lavery et al. Diabetes Care 2008]. Monitoring physical activity during drug therapy in the diabetic foot may also be a useful tool in predicting disease progression.

Are Skin Temperatures Predictive of Ulceration?
Reproduced with permission from D. Armstrong, MD.
Optimal diabetic foot management incorporates innovative strategies, such as a team approach, new technologies, and predictive risk assessment tools. Treating the acute foot wound is a complex endeavor, and preventing recurrence is an important part of successful management.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.