

Summary
This article discusses the links between fructose consumption and cardiometabolic risk, as well as the metabolic mechanisms that are associated with fructose and how they apply to cardiometabolic risk.
- Cardiometabolic Disorder
- Obesity
Another issue that merits discussion is the role of fructose consumption in cardiometabolic risk. Kimber Stanhope, PhD, University of California, Davis, CA, provided information about the metabolic mechanisms that are associated with fructose and how they apply to cardiometabolic risk. Studies have shown that diets that are high in fructose induce symptoms of the metabolic syndrome in animals [Bizeau ME et al. Metabolism 2005; Havel PJ et al. Nutr Rev 2005; Le KA et al. Curr Opin Clin Nutr Metab Care 2006; Wei Y et al. J Nutr Biochem 2007]. In animals, diets that are high in fructose have been found to increase de novo lipogenesis, dyslipidemia, insulin resistance, and obesity. However, few studies are available with regard to the impact of fructose on these metabolic components in humans.
A recent study by Stanhope and colleagues investigated the effect of fructose consumption on body composition, de novo lipogenesis, lipids, and insulin sensitivity compared with glucose in overweight/obese humans. Over the course of 10 weeks, patients consumed either fructose- or glucose-sweetened beverages, providing 25% of energy requirements. Two of the 10 weeks were part of an inpatient intervention period, allowing for comparisons under well-controlled metabolic conditions (with a coordinated energy-balanced diet), and 8 of the 10 weeks were part of an outpatient intervention period that included an ad libitum diet along with the predetermined beverage component of the diet. All patients were aged 40 to 72 years with a BMI of 25 to 35 kg/m2 and stable body weight 6 months prior to study participation.
Visceral adipose tissue accumulation increased significantly in patients who consumed fructose versus glucose at 10 weeks (p<0.01) suggesting differential effects of fructose versus glucose on regional adipose distribution. Consumption of fructose led to dyslipidemia, but lipids did not appear to be influenced by the consumption of glucose. Increased levels of postprandial triglycerides, fasting and postprandial apoB and LDL, fasting small dense LDL, and oxidized LDL were observed in the fructose group versus no change in the glucose group. Fructose consumption was also associated with deteriorated glucose tolerance and insulin sensitivity. At 10 weeks, insulin sensitivity was decreased by 17% in the fructose group [Stanhope KL et al. J Clin Invest 2009].
It is important to note that foods are generally sweetened with sucrose (which is 50% fructose/50% glucose) or high-fructose corn syrup (which is 42% to 55% fructose/remaining % glucose) rather than pure fructose or pure glucose. Therefore, more studies are needed to determine the effects of consuming diets that are high in sucrose or high-fructose corn syrup and to determine the level of dietary fructose that can be consumed without adverse metabolic effects.
Julie Miller-Jones, PhD, St. Catherine University, St. Paul, MN, emphasized the importance of differentiating between fructose sources, such as fruits and vegetables, versus added fructose that is ingested in the form of corn syrup, high-fructose corn syrup, and agave.
Some of the trends that are noted with sweetened beverage consumption may be the result of increased caloric intake. In a study by Ludwig and colleagues, the consumption of sweetened beverages predicted weight gain in children [Ludwig et al. Lancet 2001]. Investigators concluded that weight gain may have less to do with the type of sweetener and may be more closely related to excess calories. In an evidence-based review by Dolan and colleagues, the physiological effects (higher triglycerides and weight gain) that are observed with very high fructose intake were not observed with fructose intake that approached the 95th percentile [Dolan et al. Crit Rev Food Sci Nutr 2010].
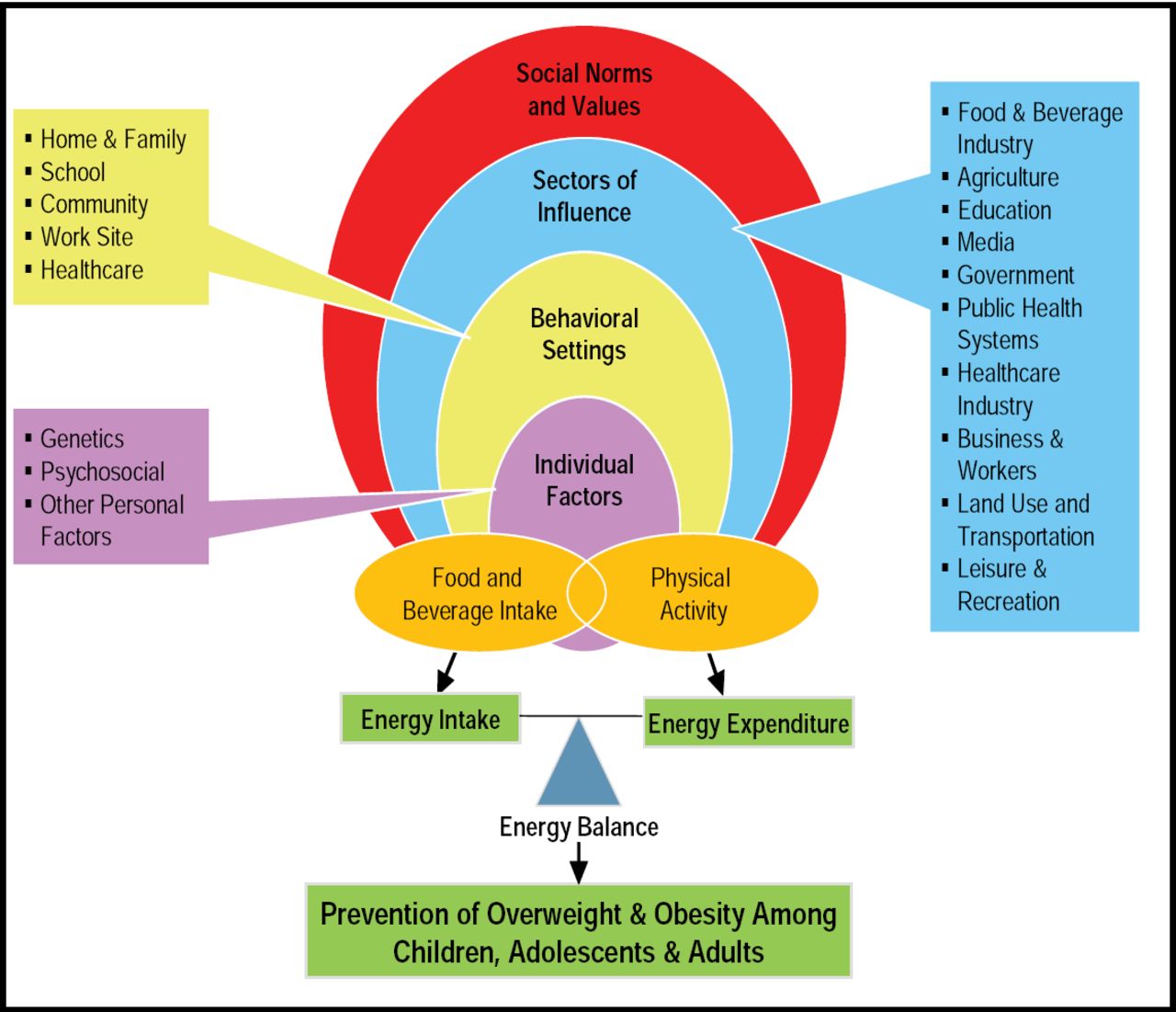
Michele M. Doucette, PhD, University of Colorado, Denver, CO, explained that added sugars can be consumed in moderation as part of a balanced diet and active lifestyle, provided that an individual's required total caloric intake is taken into account. Numerous environmental factors should also be considered when counseling patients, including behavioral settings, socioeconomic status, physical activity, and genetics (Figure 1).

Socioecological Framework for Preventing Obesity.
Reproduced with permission from M. Doucette, PhD.
The American Heart Association recommends limiting daily added sugar (based on the 2005 Dietary Guidelines daily discretionary calories) to ≤100 calories (6 tsp, 25 g) for women and ≤150 calories (9 tsp, 38 g) for men [Johnson RK et al. Circulation 2009]. Limiting added sugars and avoiding sugar-sweetened beverages (currently estimated to be 30% of total added sugar intake) may help reduce cardiometabolic risk and obesity [Malik VS et al. Circulation 2010].
Finally, the recent science shows us that a multifaceted approach is needed to help stem the tide of cardiometabolic risk in our patients.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.