

Summary
Cardiovascular disease (CVD) is one of the primary clinical risks that are associated with type 2 diabetes. While a clear graded association of CVD risk has been noted with hyperglycemia, the role of glucose control in CVD risk mitigation remains uncertain. This article discusses data from the UK Prospective Diabetes Study [UKPDS] Group, the relationship between atherosclerosis and diabetes, the ARBITER 6-HALTS Trial, and blood glucose control by sulphonylureas or insulin.
- prevention & screening
- cardiometabolic disorder
- hyperglycemia/hypoglycemia
- lipid disorders
- diabetes mellitus
Cardiovascular disease (CVD) is one of the primary clinical risks that are associated with type 2 diabetes. While a clear graded association of CVD risk has been noted with hyperglycemia, the role of glucose control in CVD risk mitigation remains uncertain. This issue was addressed by Darren K. McGuire, MD, University of Texas Southwestern Medical Center, Dallas, TX. Referencing data from the UK Prospective Diabetes Study (UKPDS) Group, Dr. McGuire noted that intensive blood glucose control by either sulphonylureas or insulin substantially decreased the risk of microvascular complications, but not macrovascular disease, in patients with type 2 diabetes [UKPDS Group. Lancet 1998].
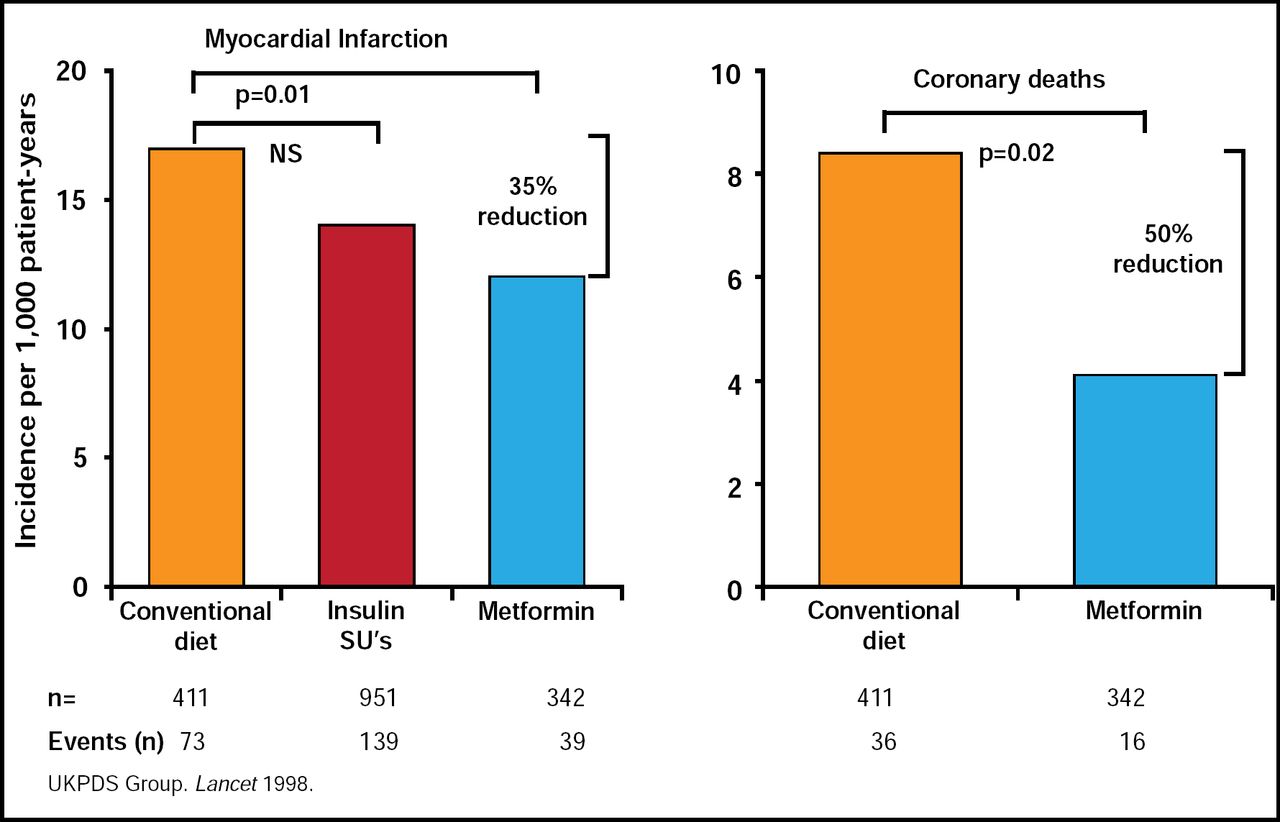
Another study from this same group investigated whether intensive glucose control with metformin attenuated the risk of heart attacks [UKPDS Group. Lancet 1998]. Compared with the conventional treatment group, patients who were allocated to metformin had risk reductions of 32% (95% CI, 13 to 47; p=0.002) for any diabetes-related endpoint (need to list components), 42% for diabetes-related death (p=0.017), and 36% for all-cause mortality (p=0.011). Among patients who were allocated to intensive blood glucose control, metformin showed a greater effect than chlorpropamide, glibenclamide, or insulin for any diabetes-related endpoint (p=0.0034), all-cause mortality (p=0.021), and stroke (p=0.032) [UKPDS Group. Lancet 1998]. A meta-analysis of five trials confirmed these findings. Intensive glycemic control resulted in a 17% reduction in events of nonfatal myocardial infarction (OR, 0.83; 95% CI, 0.75 to 0.93) and a 15% reduction in coronary heart disease events (OR, 0.85; 95% CI, 0.77 to 0.93) but no significant effect on events of stroke or all-cause mortality [Ray KK et al. Lancet 2009].

UKPDS Metformin Substudy: CHD Events.
Reproduced with permission from D. McGuire, MD.
As the prevalence of diabetes approaches 10% of the population of the United States and the number of antihyperglycemic medications on the market increases, there are converging pressures for regulatory changes. In part, this has been driven by concerns that some of these therapies may be associated with increased cardiovascular risk. Guidance from the US FDA to the industry states that “sponsors should demonstrate that the therapy will not result in an unacceptable increase in cardiovascular risk.”
Atherosclerotic disease is prevalent in diabetic patients and accounts for significant morbidity and mortality. Danielle Duffy, MD, Thomas Jefferson University, Philadelphia, PA, discussed the appropriate lipids goals for diabetic patients and how to achieve them.
The Adult Treatment Panel III of the National Cholesterol Education Program issued an evidence-based set of guidelines on cholesterol management in 2001 that confirmed the benefit of cholesterol-lowering therapy in diabetic patients. The guidelines support a treatment goal of low-density lipoprotein cholesterol (LDL-C) <100 mg/dL in this population, as this population are felt to be at equivalent risk to patients with known cardiovascular disease.
Large-scale clinical trials and a meta-analysis [Sattar N et al. Lancet 2010] confirmed the benefits of statin use in diabetic patients to lower lipids. In one study, 40 mg simvastatin daily reduced the rate of first major vascular events by about 25% in a wide range of diabetic patients [Collins R et al. Lancet 2004]. Niacin treatment, added to statin monotherapy to further modify the lipid profile (raise HDL, further reduce triglycerides and LDL), caused a significant regression of carotid intima-media thickness in the ARBITER 6-HALTS trial [Taylor AJ et al. N Engl J Med 2009].
In summary, Dr. Duffy noted that a target LDL-C <70 mg/dL remains the primary lipid goal for patients with diabetes, with statins the first-line choice for lipid lowering.
A target-driven, long-term, intensified intervention that is aimed at multiple risk factors in patients with type 2 diabetes and microalbuminuria has been shown to reduce the risk of cardiovascular and microvascular events by about 50% [Gaede P et al. N Engl J Med 2003]. Donna M. Polk, MD, University of California, Los Angeles, CA, outlined such an intervention strategy, known as the ABCs of care for providers of diabetic patients.
ABCs of Care for Providers of Diabetic Patients.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.