

Summary
The 1999 consensus recommendations for heart failure (HF) stated that obese patients should lose weight [Am J Cardiol 1999], and according to data from the Framingham Heart Study, even being overweight poses an increased risk for HF (5% for men and 7% for women for each increment of 1 in body mass index) [Kenchaiah S et al. N Engl J Med 2002]. However, the current American College of Cardiology/American Heart Association Heart Failure Guidelines [Hunt SA et al. J Am Col Cardiol 2005; Jessup M et al. Circulation 2009] contain no mention of weight loss for HF patients. Why? This article discusses clinical trials why fatter may be better in heart failure.
- heart failure
- cardiometabolic disorder
- obesity
The 1999 consensus recommendations for heart failure (HF) stated that obese patients should lose weight [Am J Cardiol 1999], and according to data from the Framingham Heart Study, even being overweight poses an increased risk for HF (5% for men and 7% for women for each increment of 1 in body mass index [BMI]) [Kenchaiah S et al. N Engl J Med 2002]. However, the current American College of Cardiology/American Heart Association Heart Failure Guidelines [Hunt SA et al. J Am Col Cardiol 2005; Jessup M et al. Circulation 2009] contain no mention of weight loss for HF patients. Why? According to Tamara Horwich, MD, UCLA, Los Angeles, CA, fatter is better in heart failure.
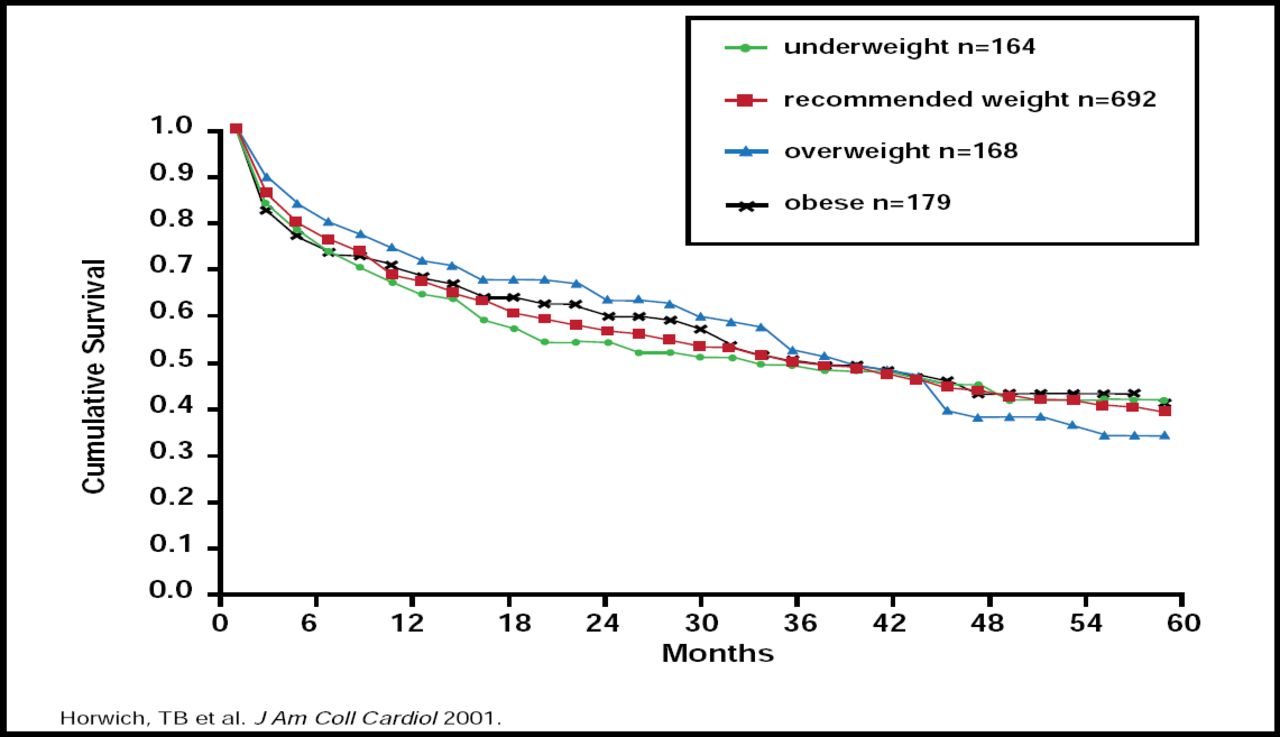
The relationship between weight and HF was first investigated more than 10 years ago in a study that included 1203 patients with advanced systolic HF. The results of that study showed that obesity is not associated with increased mortality and, in fact, may confer a more favorable prognosis, despite the fact that the obese and overweight patient groups had significantly higher rates of hypertension and diabetes, as well as higher levels of cholesterol, triglycerides, and low-density lipoprotein cholesterol (Figure 1) [Horwich TB et al. J Am Coll Cardiol 2001]. These results were recently confirmed in a meta-analysis of nine observational studies (n=28,209) in which both obesity and being overweight were associated with lower all-cause and cardiovascular mortality rates compared with normal weight patients with CHF and were not associated with increased mortality in any study [Oreopoulos A et al. Am Heart J 2008].

Adjusted Survival Analysis: Overweight and Obese Fair Better.
Copyright © 2001 American College of Cardiology. All rights reserved.
Paradoxically, low body mass index (BMI) may be associated with poorer survival in patients with chronic heart failure (CHF). In the Candesartan in Heart failure: Reduction in Mortality and Morbidity (CHARM) study, CHF patients with ≥5% weight loss in 6 months had more than a 50% increase in mortality compared with those with stable weight. The risk increased more than four-fold for patients whose last recorded annual weight loss exceeded 10%. Weight loss accelerated in the year prior to death [Pocock SJ et al. Eurt Heart J 2008]. This reversal has been termed the “obesity paradox.”
Several explanations for the obesity paradox in HF patients have been offered: obese HF patients are simply less sick because they present at an earlier stage of disease; high BMI represents greater metabolic reserve in HF; and/or obesity (increased fat or increased lean mass) is protective in terms of altering neurohormonal, inflammatory cytokine, and adipokine physiology [Von Haehling S et al. Circulation 2007].
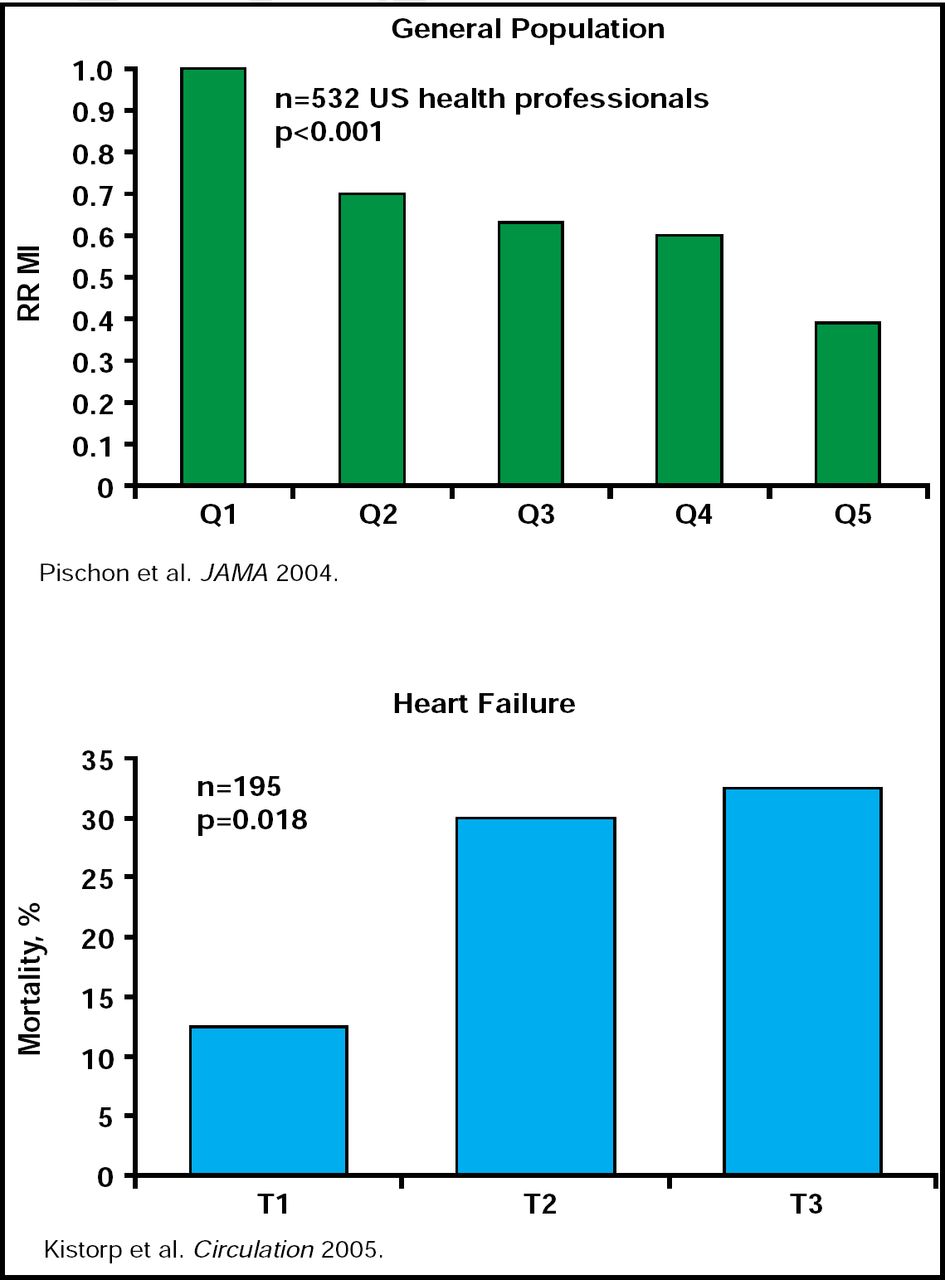
The neurohormonal connection has been evaluated in several studies. Obese individuals tend to have low levels of adiponectin, an adipocyte-derived peptide with insulin-desensitizing and anti-inflammatory properties. In the general population, low levels of adiponectin are associated with a higher risk of MI; however, in HF, the opposite is true—low levels of adiponectin are associated with decreased mortality (Figure 2) [Pischon T et al. JAMA 2004]. Another neurohormone that is altered with respect to BMI is brain natriuretic peptide (BNP). HF patients with a BMI <25 have higher levels of BNP compared with overweight (BMI 25 to 29.9) and obese HF patients (BMI ≥30) [Horwich T et al. J Am Coll Cardiol 2006]. However, in the general population, low BNP levels are generally associated with lean body mass [DAS SR et al. Circulation 2006]. This leads to the question of whether it is lean body mass that is offering cardiovascular protection in overweight and obese HF patients. The answer is important, because almost all of the studies of obesity and HF use BMI as a measure, and while BMI does correlate with fat mass, it can not discriminate between lean mass and fat mass [Romero-Corral A et al. Int J Obesity 2008].

Adiponectin Levels.
Reproduced with permission from T. Horwich, MD.
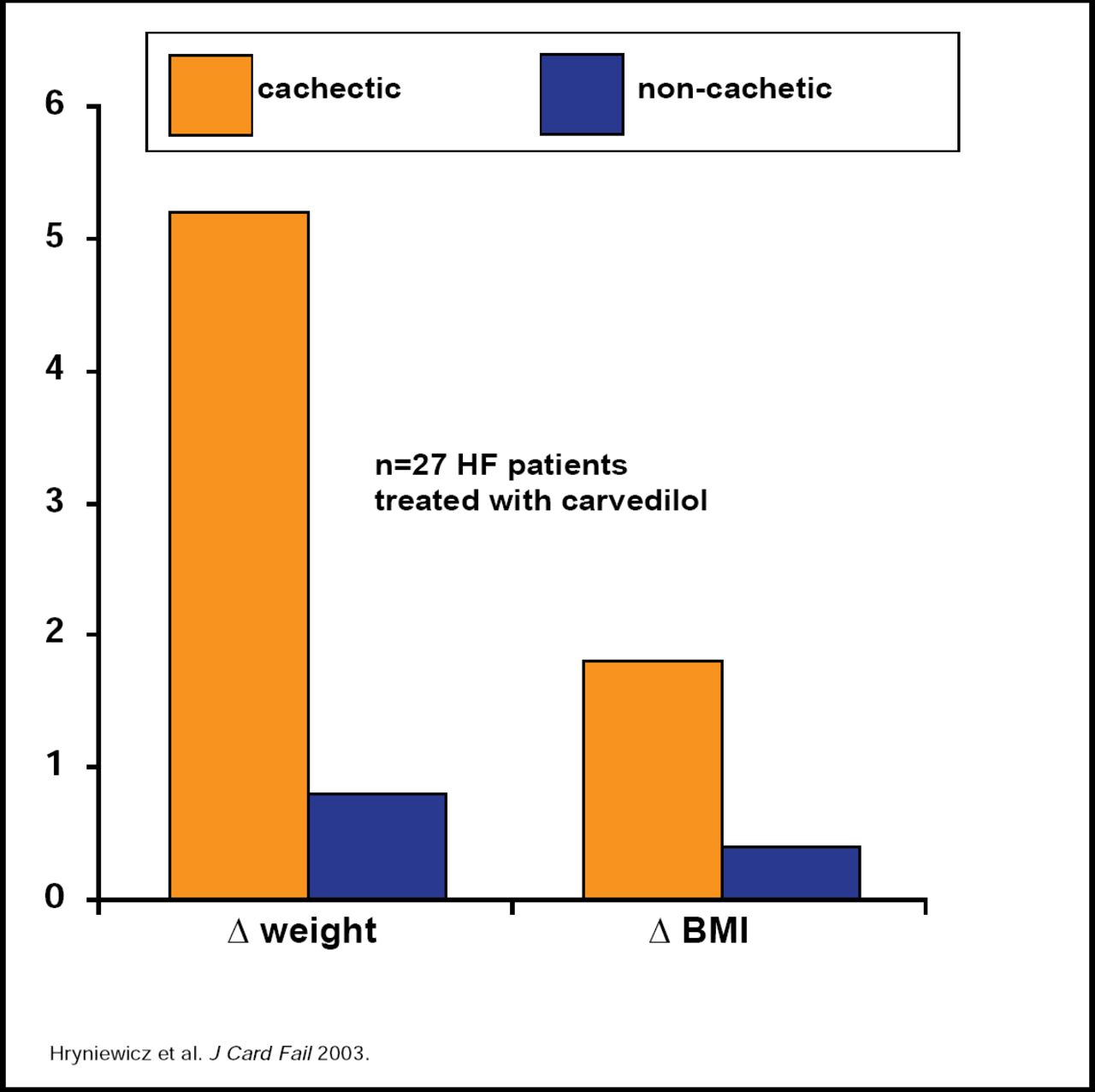
If the paradox implies that being overweight or obese is associated with improved outcomes and if unintentional weight loss portends poor prognosis in HF patients, what are the clinical implications? Dr. Horwich suggests that currently used HF medications, such as ACE inhibitors and beta-blockers, prevent weight loss (Figure 3), and traditional dietary advice that includes the restriction of fluids, salt, alcohol, high K foods, and sugar if the patient is also a diabetic, but not weight reduction. More specifically, for HF individuals with a BMI:
-
<30 kg/m2 – do not encourage weight loss
-
>40 kg/m2 – lose weight to BMI <40
-
30 to 40 kg/m2 – inconclusive evidence to make recommendation
The best survival has been found for patients with a BMI of 30 to 32 kg/m2 [Riegel B et al. Circulation 2009].

Impact of ACEIs and Beta-Blockers.
Reproduced with permission from T. Horwich, MD.
The findings of the obesity paradox extend beyond HF to other chronic conditions, such as end-stage renal disease, rheumatoid arthritis, chronic obstructive pulmonary disease, AIDS, malignancy, and coronary artery disease, as well as in the elderly in general. More studies are needed to determine whether weight loss promotion in patients with HF is a worthwhile goal or may even be harmful. In addition, we need studies to determine what impact intentional weight gain, exercise to increase muscle mass, and nutritional therapy have in HF patients with low BMI.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.