

Summary
Although technical advances in the surgical management of aneurysms are limited, microsurgery can still be used to create elegant and anatomical bypasses in the hands of a skilled neurosurgeon. The evolving trends in the field include more minimally invasive approaches; more use of direct clipping, clip reconstruction, and bypass procedures; and less brain retraction and skull base surgery. Circulatory arrest as part of the aneurysm surgical process is no longer used.
- interventional techniques & devices
- ischemia
Although technical advances in the surgical management of aneurysms are limited, microsurgery can still be used to create elegant and anatomical bypasses in the hands of a skilled neurosurgeon, said Michael Lawton, MD, University of California, San Francisco, CA. The evolving trends in the field include more minimally invasive approaches; more use of direct clipping, clip reconstruction, and bypass procedures; and less brain retraction and skull base surgery. Circulatory arrest as part of the aneurysm surgical process is no longer used.
Dr. Lawton said that direct clipping is the best mechanical repair of an aneurysmal defect, because it closes the aneurysm neck, apposes normal arterial tissue, reinforces the bifurcation, allows for contoured reconstruction, and offers great treatment durability overall. For unclippable aneurysms, intracranial-intracranial (IC-IC) bypass is now the preferred approach. IC-IC does not require a donor harvest or neck incision, the graft is short, and the repair is less vulnerable, as the entire procedure is kept inside the cranium. IC-IC bypass may take the form of side-to-side anastomosis (in situ bypass), end-to-end (reanastomosis), end-to-side (reimplantation), or the use of a graft. On the negative side, IC-IC requires temporary occlusion of two arteries versus one with the extracranial (EC)-IC procedure and is a more technically difficult procedure. Sites that are favorable for IC-IC bypasses are the Sylvian fissure, interhemispheric fissure, carotid and crural cisterns, and cisterna magna. Outcomes appear comparable with those that employ an EC-IC approach.
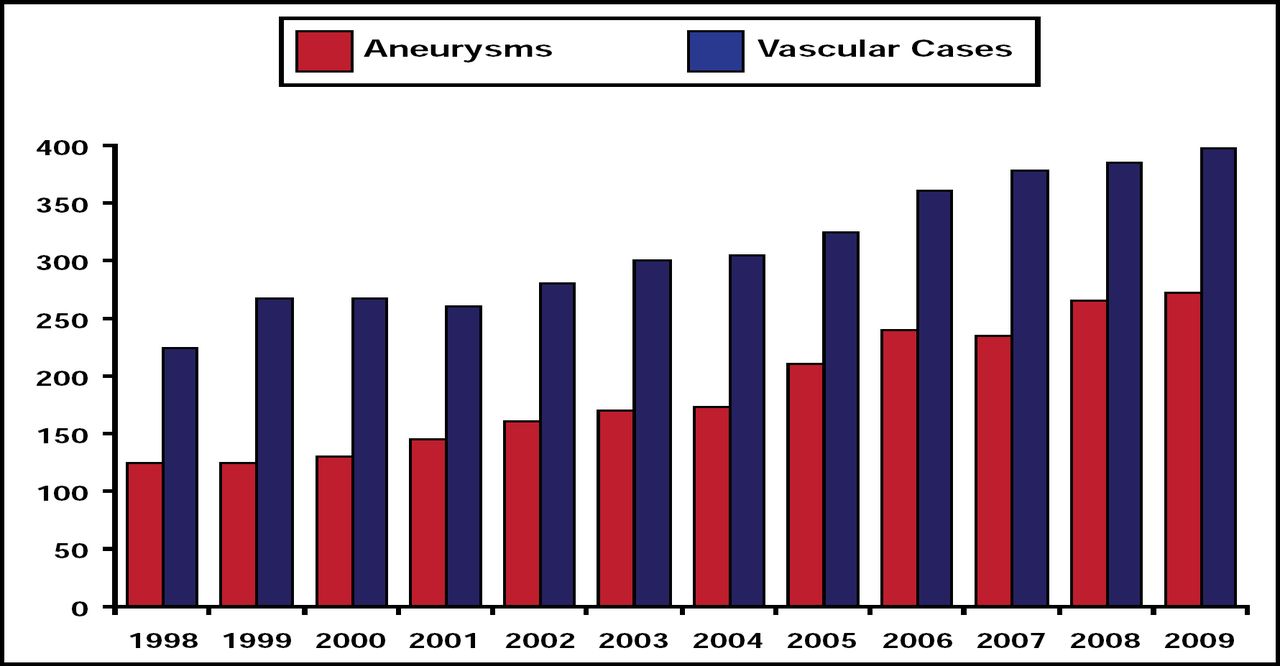
“Aneurysm surgery is increasing,” said Dr. Lawton, “and aneurysm surgeons are needed to meet this rising demand,” (Figure 1).

UCSF Aneurysm Surgery.
Reproduced with permission from M. Lawton, MD.
Saruhan Cekirge, MD, Hacettepe University Hospital, Ankara, Turkey, discussed advanced approaches for the endovascular treatment of cerebral aneurysms. Since his pioneering work, which combined a metallic stent with a liquid polymer (ONYX liquid embolic system) for treating giant intracranial aneurysms [Cekirge et al. Neuroradiology 2006], new access devices and endovascular tools have become available not only for proximal but also for distal aneurysms. Parent artery reconstruction has been improved with the use of intracranial stents, liquid embolic ONYX, and liquid-coil and/or stent-combined treatments that are aimed at treating not only the aneurysm sac but also the sick vessel wall that is adjacent to the aneurysm neck [Cekirge S. & Saatci I. J Neurosurg 2006]. This makes it possible to change the sick parent artery and exclude the aneurysm from circulation using stent grafts with a novel technique, described by Ankara-Hacettepe and colleagues [Saatci-Cekirge et al. AJNR 2004]. This new technique has been widely accepted as a starting point of the new flow diversion avenue in the endovascular aneurysm treatment.
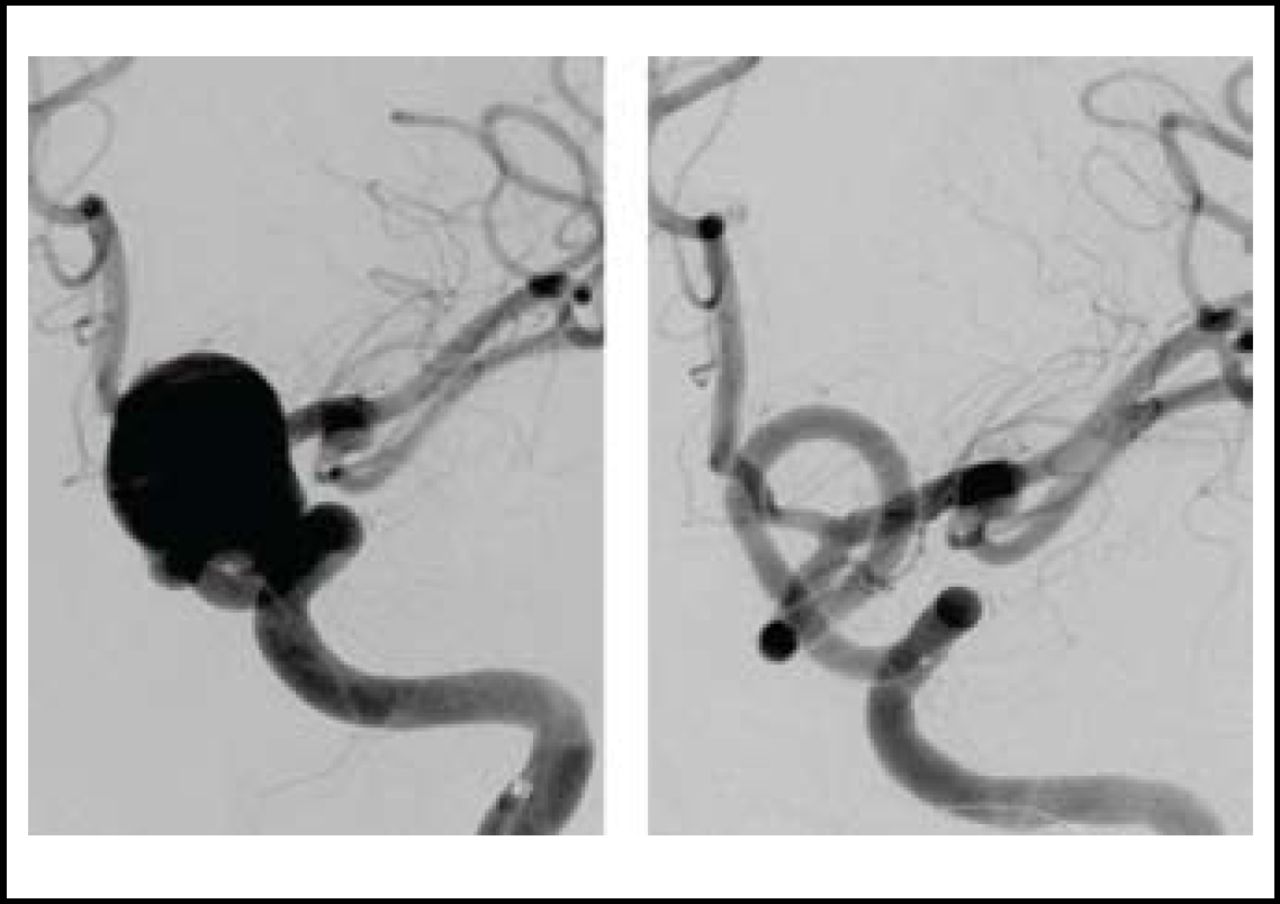
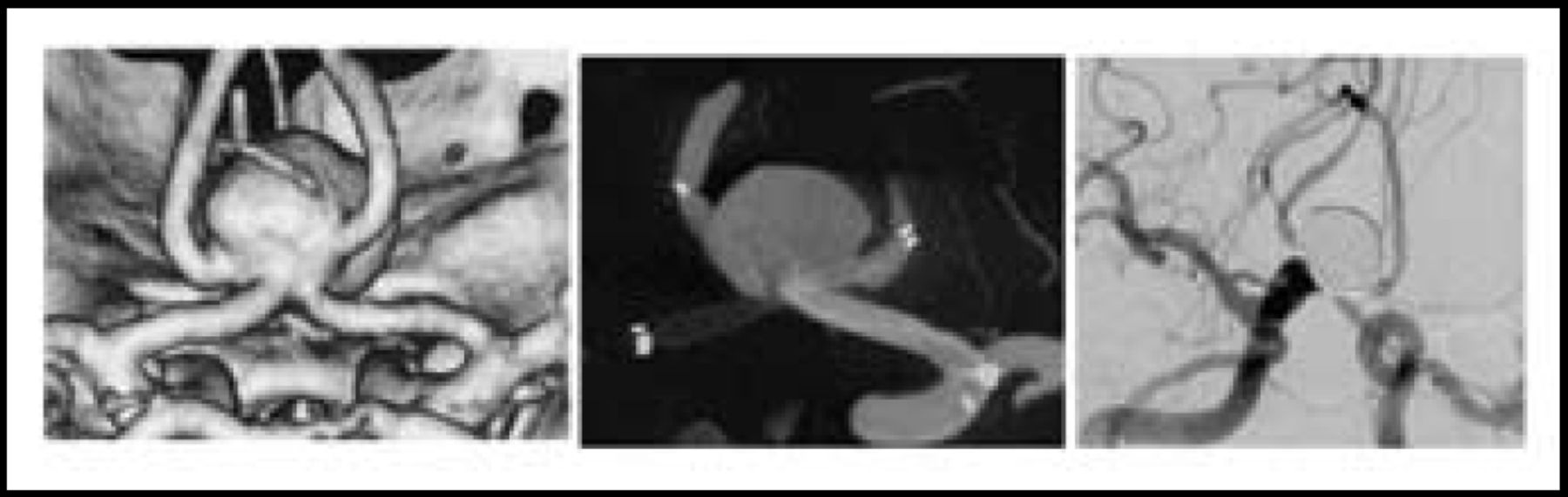
Success has also been achieved with self-expandable stents and flow diversion techniques with no endosaccular packing. Flow diversion can be achieved with telescopic stenting using regular self-expandable stents (stent-in-stent) and Y stenting in bifurcations or with the use of dedicated flow divertors (PIPELINE ED, SILK Stent; Figure 2). Y or X (Figure 3) stenting reconstruction with coiling of complex distal bifurcation aneurysms created a revolutionary procedure, and many so-called ‘surgical’ aneurysms are now being managed endovascularly. Follow-up studies have shown remarkable success with these techniques. In 72/94 aneurysms cases, some that were followed for up to 2 years, angiography indicated that all had complete occlusion with no recurrences and significant parent artery stenosis. In 4 aneurysms, a nonsignificant stenosis was observed in one distal edge of a stent.

Giant ICA Aneurysm Treated with Pipeline Flow Divertor and 6-Month Control Angiography Showing Excellent Reconstruction of the Artery Without Sac Coiling.
Reproduced with permission from S. Cekirge, MD.

X Stenting Reconstruction of a Complex A Com Aneurysm With 2-Year Follow-Up Angiography.
Reproduced with permission from S. Cekirge, MD.
The mortality and morbidity rates that are associated with these new endovascular treatments are superior to those that are associated with surgical clipping of giant aneurysms. Prof. Cekirge believes that these techniques have significant potential for the reconstructive treatment of intracranial aneurysms.
Intracranial aneurysms (IA) are a significant problem, affecting 2% to 5% of the population. Worldwide, ∼500,000 hemorrhagic strokes occur annually with devastating consequences: 45% of patients die within a month; 30% never make it to the hospital; and 50% of the survivors are left with severe neurological deficits, requiring long-term care [Brisman JL et al. N Engl J Med 2006]. Typically, there are no antecedent events or warning signs. Although surgical or endovascular repair can prevent morbidity and mortality, unless we develop a reliable way to diagnosis an aneurysm prior to rupture, there is little that we can do, said Murat Gunel, MD, Yale University School of Medicine, New Haven, CT.
Epidemiological studies that have shown that siblings of patients with an IA have a 4-fold increased risk of hemorrhagic stroke due to IA [Schievink WI et al. J Neurosurg 1995] tell us that we can use genetic studies to identify the mechanistic pathways that lead to the formation of these aneurysms. Recently, a candidate gene study reported a common sequence variant on chromosome 9p21, tagged by rs10757278-G, to be associated with, in addition to coronary artery disease (CAD) and abdominal aortic aneurysm, intracranial aneurysms (OR=1.29, P=2.5 × 10-6) [Helgadottir A et al. Nat Genet 2008].
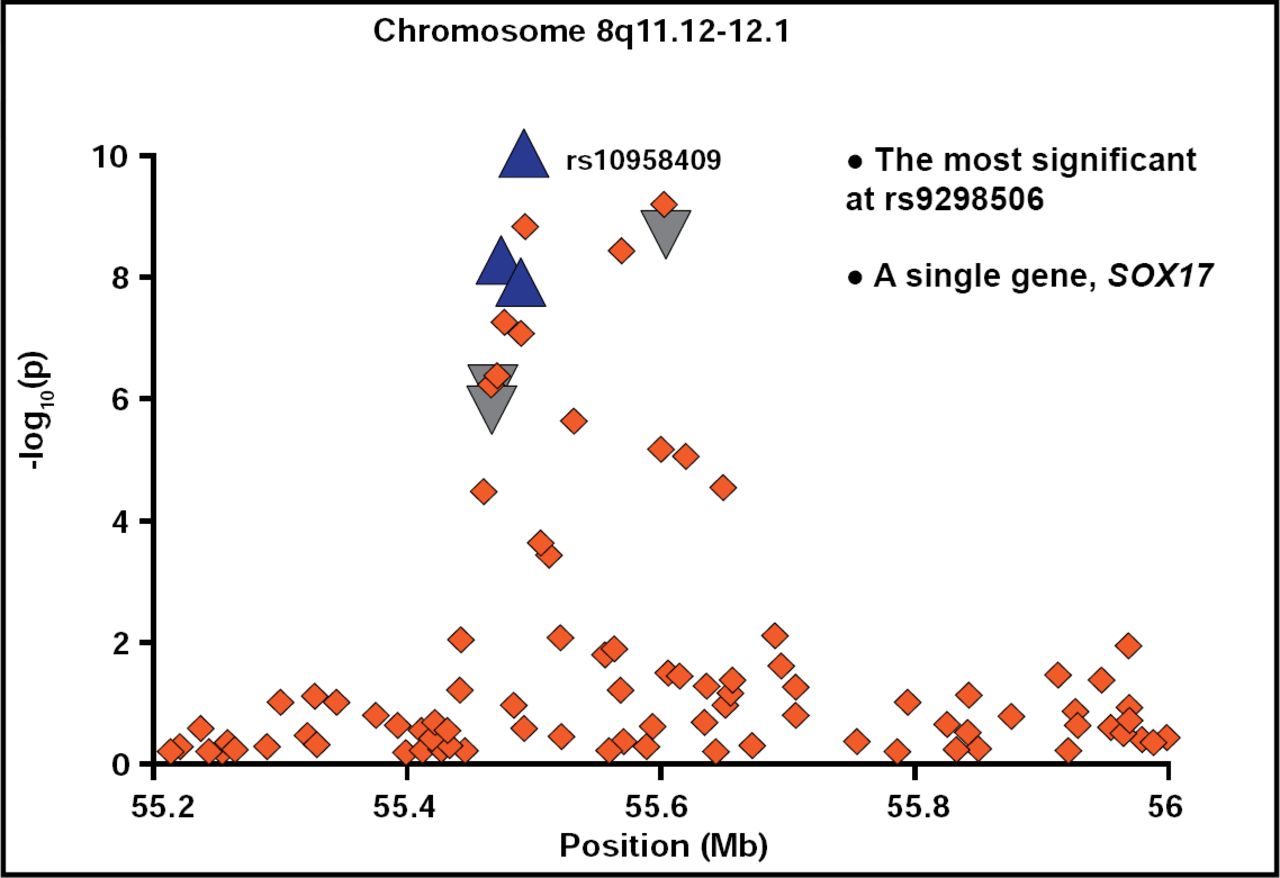
This was followed by an independent genomewide association study (GWAS), based on genotyping of >300,000 SNPs in ∼1700 cases and 7300 controls in 2 genetically similar European cohorts with replication in a genetically distant Japanese cohort (495 cases/676 controls), that identified common variants that influence the occurrence and/or rupture of IAs [Bilguvar K et al. Nat Genet 2006]. Initially, significant associations were noted on chromosomes 1, 2, 8, and 9. However, when the study population was expanded to include ∼5500 cases and 12,000 controls from the United States, European, and Japanese cohorts, significant heterogeneity was noted among the cohorts. Chromosomes 1 and 2 lost significance, and 8 and 9 increased in significance, suggesting that they contain aneurysm susceptibility genes. Replication was particularly significant at location rs9298506, which is near a single gene called SOX17, essential for the specification and maintenance of the endoderm of the embryo [Hudson C et al. Cell 1997]. The SOX transcription factor family plays a key role in the generation and maintenance of fetal and neonatal stem cells for both the hematopoietic and endothelial lineages [Kim I et al. Cell 2007] that also play a role in intracranial postnatal angiogenesis in mice [Matsui T et al. J Cell Sci 2006]. A strong association with chromosome 9 that was previously shown to be associated with CAD was also confirmed (Figure 4) [Samani NJ et al. N Engl J Med 2007].

Chromosome 8.
Reproduced with permission from M. Gunel, MD.
For the chromosome 9p21 locus, the cyclin-dependent kinase inhibitor p16INK4a was identified as a possible target. This protein plays a role in the regulation of stem cell populations, including bone marrow-derived cells of the vasculature [Janzen V et al Nature 2006]. Inhibition of p16INK4a may ameliorate the physiological impact of aging on stem cells and thereby improve vascular injury repair in aged tissue.
Based on these findings, it was hypothesized that IA results from defective development and/or repair of the vasculature through the progenitor cell populations. Vascular injury mobilizes bone marrow or vasculature-derived progenitor/stem cells that localize to sites of damage, and these cells appear to be important in the repair process [Werner N et al. Arterioscler Thromb Vasc Biol 2002]. Thus, IA gene variants might be involved in the maintenance and proliferation of progenitor cells and the vascular repair process.
It is hoped that further efforts to determine the role of these genes in the maintenance of the vascular repair pathway will provide new therapeutic opportunities in IA treatment.

The editors would like to thank the many members of the American Stroke Association presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.