

Summary
The neurodevelopmental sequelae of congenital heart disease and its treatment are likely to limit the ultimate educational achievements, employability, insurability, and quality of life for these children. The effects include cognitive deficits, such as a short attention span, delays in the development of motor skills, speech, and language; and impaired social competency and executive functions.
- cerebrovascular disease
- prevention & screening
- thrombotic disorders
The neurodevelopmental sequelae of congenital heart disease (CHD) and its treatment are likely to limit the ultimate educational achievements, employability, insurability, and quality of life for these children, said J. William Gaynor, MD, Children's Hospital of Philadelphia, PA. The effects include cognitive deficits, such as a short attention span, delays in the development of motor skills, speech, and language; and impaired social competency and executive functions.
Children with CHD are at risk for stroke before and after surgery and even later in life. The frequency of vaso-occlusive stroke in children with CHD who undergo cardiac surgery is 5.4 cases per 1000 children. Age, duration of bypass, and reoperation may be associated with stroke risk [Domi T et al. Pediatrics 2008]. There remains an unmet need for data that concern the long-term prevalence of or specific risk factors for stroke, as well preventative therapies in the CHD population, concluded Dr. Gaynor.
The issue of whether to use antithrombotic therapy for stroke prevention in children with CHD remains unanswered due to a lack of data, said Fenella J. Kirkham, MD, UCL Institute of Child Health, University College London, London, UK. However, there is a 6-fold increased risk of stroke for these children compared with the general population [Fox C. 2010 unpublished]. According to Prof. Kirkham, although primary prevention may be difficult, we may be able to prevent recurrence if we understand the mechanisms, which include primary arterial disease, such as dissection and moyamoya, and cerebral sinovenous thrombosis, as well as embolus. Appropriate management of risk factors is then possible.
For all children with arterial ischemic stroke, including those with cardiac disease, the risk of clinical recurrence is increased in children with moyamoya and other vasculopathies and in those with genetic thrombophilia and raised lipoprotein (a) (Table 1).
Multivariate Cox Regression for Risk of Recurrent Stroke in AIS.
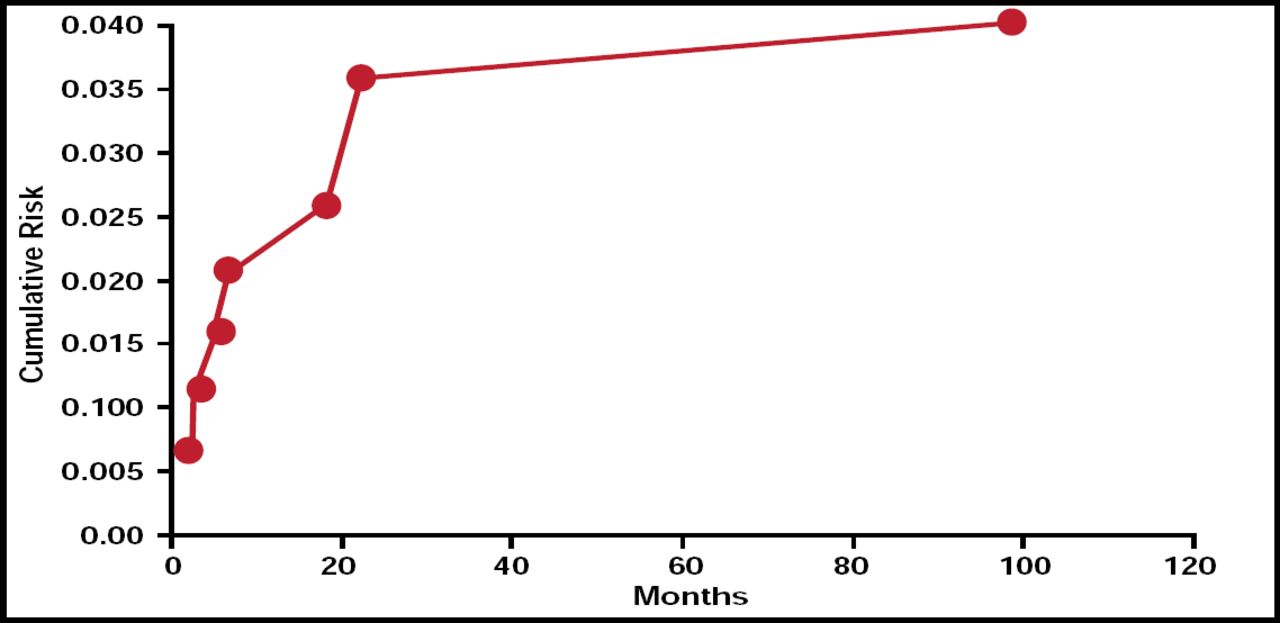
Recurrent thromboembolism in neonates is very low and occurs in the first year of life (Figure 1) [Gunther G et al. Stroke 2000]. Risk factors for recurrent sinovenous thrombosis include older age, presence of thrombophilia, and failure to recanalize affected venous sinuses. The current guidelines allow for anticoagulation of these patients. Prof. Kirkham is less inclined to use anticoagulation except in these children. She suggests the use of aspirin but would also exclude or treat iron deficiency. She cautions that before beginning therapy, it is important to fully investigate the patient.

Recurrent Thromboembolism in Neonates.
Reproduced with permission from F. Kirkham, MD.
There is a reasonably well-established link between patent foramen ovale (PFO) and cryptogenic stroke in young patients, according to Steven Messé, MD, Hospital of the University of Pennsylvania, Philadelphia, PA. However, the risk of recurrent stroke is relatively low (∼1.5% per year on aspirin), while percutaneous PFO closure is expensive, has a small but real risk of complication, does not replace other medical therapy, and is unproven.
The combination of PFO and atrial septal aneurysm (ASA) was associated with an increased risk of recurrent stroke in patients (OR 3.1; 95% CI, 2.3 to 4.2) in one Class I study but not in two other subsequent Class I studies.
The medical treatment options for PFO patients include antiplatelet drugs or anticoagulation, and there are no high-level data that confirm the superiority of either of these approaches, though anticoagulation is associated with more bleeding complications. Surgical or percutaneous closure can also be performed, but this does not preclude long-term medical therapy. At this time, there are no high-level data that support PFO closure. Randomized controlled trials are ongoing, but enrollment has been slowed by rampant use of off-label devices for PFO closure. Despite the lack of evidence, percutaneous septal closure procedures increased 50 times between 1998 and 2004.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.