

Summary
This article discusses the prevention, management, and processing of intracerebral hemorrhage (ICH), as well as key clinical trials concerning the surgical management of ICH. This article also reviews the tools and procedures for recovery and prevention of ICH recurrence.
- ischemia
- interventional techniques & devices
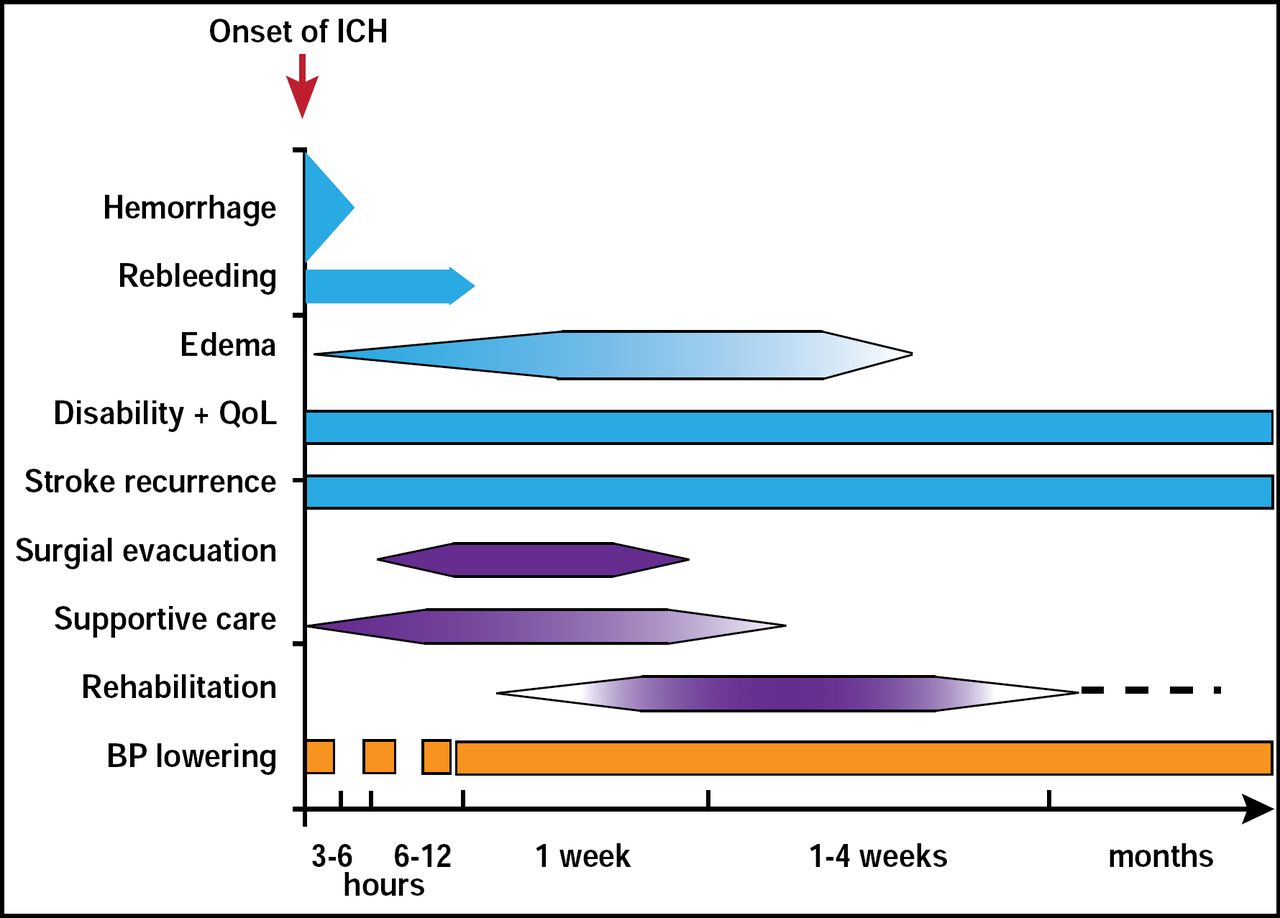
Craig Anderson, MD, University of Sydney, Sydney, Australia, noted that the best “treatment” for intracerebral hemorrhage (ICH) is prevention but that a good understanding of the early natural history of ICH and subsequent bleeding is needed before specific treatment remedies can be applied. To illustrate, he noted that there is substantial growth in the volume of parenchymal hemorrhage between baseline and 24-hour CT scans in more than one-third of ICH patients and that this early clot growth is associated with more frequent neurological deterioration [Brott T et al. Stroke 1997]. Within days of the initial hemorrhage, intracranial pressure increases, followed by hydrocephalus and chemical meningitis, and later, toxicity from iron and hemoglobin breakdown products occurs. The degree and growth in perihematomal edema are strongly related to the size of the underlying hematoma following acute ICH [Arima H et al. Neurology 2008]. Given this scenario, medical management of ICH patients involves active, well-organized/ coordinated management that includes assessment and monitoring, acute management (physiological control, early mobilization, managing complications, and skilled nursing), multidisciplinary rehabilitation, and discharge planning. An early CT scan (<24 hours) for diagnostic assessment is crucial. Dr. Anderson cautioned that ICH patients must be managed according to the timeline of events (Figure 1).

Management According to the Time of Events in ICH.
Reproduced with permission from C. Anderson, MD.
Joseph P. Broderick, MD, University of Cincinnati, Cincinnati, OH, used data from some of the key clinical trials in ICH [Mendelow AD et al. Lancet 2005; Teernstra O et al. Stroke 2003; Wang WZ et al. Int J Stroke 2009; Morgan T et al. Acta Neurochir Suppl 2008; Cho DY et al. Surg Neurol 2006; Hanley DF. Stroke 2009] to answer important questions that concern the surgical management of ICH—such as when surgical removal of ICH is indicated, the role of the location of the ICH in the surgical decision, the best surgical approach to remove the hemorrhage, and whether the timing of surgery matters.
Dr. Broderick concluded that clinical trial evidence and expert opinion currently indicate that:
Patients with cerebellar hemorrhage who are deteriorating neurologically or who have brain stem compression and/or hydrocephalus from ventricular obstruction should undergo surgical removal of the hemorrhage as soon as possible.
In those patients who present in coma with deep hemorrhages, removal of ICH by standard craniotomy is not recommended. Use of minimally invasive approaches in these patients is under study. For patients who present with lobar clots ≤1 cm from the surface, evacuation of supratentorial ICH by standard craniotomy might be considered.
The effectiveness of minimally invasive clot evacuation, utilizing either stereotactic or endoscopic aspiration with/without thrombolytic usage, is uncertain. Although intraventricular administration of rt-PA in IVH appears to have a fairly low complication rate, efficacy, and safety of this treatment is uncertain.
There is no clear evidence that ultraearly removal of supratentorial ICH improves functional outcome or mortality rate. Very early craniotomy may be associated with an increased risk of recurrent bleeding.
We still need a lot more information, which may come from the clinical trials that are currently in progress, concluded Dr. Broderick.
“Prognostication matters,” said J. Claude Hemphill III, MD, University of California, San Francisco, CA. He noted, however, that prediction models and scoring systems are developed on, and apply to, populations of ICH patients, and while they are useful, their point scores can not be used with certainty in individual patients. Approximately half of all ICH-associated deaths occur in the first 2 days, and the majority (60% to 78%) of these is due to withdrawal of medical support [Hemphill JC et al. Neurology 2009; Zurasky JA et al. Neurology 2005]. Additionally, other care limitations, short of actual withdrawal of medical support, may impact outcome. For example, being treated in a hospital that uses do-not-resuscitate (DNR) orders within the first 24 hours after ICH as little as 10% more often than another hospital with a similar case mix has been shown to increase a patient's odds of dying during hospitalization by 13% (p<0.001). This is likely because early DNR use is probably a surrogate for overall aggressiveness of care [Hemphill JC et al. Stroke 2004].
While the use of DNR orders is unlikely to invalidate existing prediction models overall, it may very well impact the point estimates of outcome that are often used for individual patients. This has prompted American Heart Association ICH guidelines to recommend careful consideration of aggressive full care during the first 24 hours after ICH onset and postponement of new DNR orders during that time (Class IIb, Level of Evidence B). Dr. Hemphill concluded by repeating one of the basic tenets of care: “You have to survive in order to improve.”
Steven M. Greenberg, MD, Massachusetts General Hospital, Boston, MA, reviewed the tools and procedures for recovery and prevention of ICH recurrence.
ICH recurrence (2.1% to 3.7%/patient-year in population-based studies) is a significant factor in the recovery process. Lobar hemorrhages have a significantly higher risk of recurrence (p=0.007) than deep hemispheric or brain stem ICH [Viswanathan A et al. Neurology 2006]. Other possible risk factors for recurrence include older age, prior ICH, anticoagulation, APOE genotype, and number of microbleeds.
Blood pressure (BP) control is an important factor in preventing ICH recurrence. The Perindopril Protection Against Recurrent Stroke (PROGRESS) study established that a BP-lowering regimen of an angiotensin-converting enzyme and a diuretic can reduce stroke risk by 67% [Tzourio et al. Neurology 2008]. A reasonable BP target is <140/90 mm Hg. The recommendations for whether to use anticoagulant or antiplatelet therapy in ICH patients with indications for these treatments are not clear cut. There is a relatively strong contraindication to anticoagulants following ICH and a weaker one for antiplatelets, since antiplatelet agents are associated with a lower risk of catastrophic ICH than anticoagulants. The most favorable risk-benefit ratio is when there is a strong indication (such as the presence of atrial fibrillation) and the contraindication is weak (eg, a patient with a deep hemispheric ICH with well-controlled BP). Heavy alcohol use (>1 drink per day) should also be avoided, but there is currently insufficient evidence to withhold statins or restrict physical activity. Rehabilitation efforts should begin early, take a multidisciplinary approach, and continue as part of accelerated hospital discharge and reintegration to home environment.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.