

Summary
High oxygen extraction fraction (OEF) is detectable by positron emission tomography (PET), and superficial temporal artery to middle cerebral artery (STA-MCA) bypass surgery can be used to improve cerebral hemodynamics in stroke risk patients [Zipfel et al. Skull Base 2005]. This article discusses some of the studies that have used PET to detect OEF, including the COSS Study, WASID Trial, SAMMPRIS Study.
- neurology
- cerebrovascular disease
- interventional techniques & devices
- neuroimaging
When cerebral blood flow falls due to reduced cerebral perfusion pressure and the brain is unable to compensate through normal autoregulatory vasodilation, it can increase oxygen extraction fraction (OEF) to support normal oxygen metabolism. However, at least 2 studies have shown that a high OEF significantly increases the risk for stroke recurrence [Grubb RI et al. JAMA 1998; Yamauchi H et al. J Nucl Med 1999]. High OEF is detectable by positron emission tomography (PET), and superficial temporal artery to middle cerebral artery (STA-MCA) bypass surgery can be used to improve cerebral hemodynamics in stroke risk patients [Zipfel et al. Skull Base 2005].
Gregory J. Zipfel, MD, Washington University School of Medicine, St. Louis, MO, discussed some of the studies that have used PET to detect OEF.
The Carotid Occlusion Surgery Study (COSS) study is a randomized trial to determine if STA-MCA bypass surgery can reduce stroke risk in patients with recent symptomatic carotid occlusion and high OEF, as measured by PET. To date, 660 patients have been enrolled. The study is expected to be completed by May 2013. Moyamoya is an inherited disease that is associated with a high risk of recurrent stroke, particularly in individuals with bilateral involvement and ischemic symptoms that may be augmented with surgical revascularization [Hallemeir CL et al. Stroke 2006]. The North American Moyamoya study is an ongoing study that is attempting to identify high-risk moyamoya patients using PET-detected increased OEF to guide clinical management.
Felipe C. Albuquerque, MD, Barrow Neurological Institute, Phoenix, AZ, reviewed surgical approaches for basilar artery reconstruction. Patients with basilar occlusion are 2.5 times more likely to have a poor outcome compared with those who have basilar stenosis. Conventional treatment (eg, antiplatelets, anticoagulation, or both) of symptomatic basilar artery occlusion is associated with a poor outcome in almost 80% of patients [Schoneville WJ et al. J Neurol Neurosurg Psychiatry 2005]. Neither a local intra-arterial thrombolysis (IAT) nor intravenous thrombolysis (IVT) approach seems to improve mortality or morbidity. Death and dependency are equally common (78% [59 of 76] and 76% [260 of 344], respectively; p=0.82). Only 24% of patients who were treated with IAT and 22% who were treated with IVT reached good outcomes [Lindsberg P & Mattle HP. Stroke 2006].
Recanalization may be an option. In data that were presented by Dr. Albuquerque from his own clinic, of 10 patients who were treated with angioplasty and/or stenting, 7 improved or were stable and 3 died.
In another study, despite a significant incidence of ischemic and nonischemic complications after basilar artery stent placement, most patients achieved freedom from vertebrobasilar ischemia and good-to-excellent clinical outcomes (9 of 10 patients) at late midterm follow-up (12 to 46 months) [Abruzzo TA et al. Am J Neuroradiol 2007].
The complete occlusion of the basilar artery has a poor natural history despite the best medical management. It is a different disease state than acute occlusion in that it has a longer course to presentation due to the presence of some collateral flow around the occlusion. Recanalization may improve outcomes in certain individuals if a steady state of patency can be achieved. However, Dr. Albuquerque believes that it is imperative that the patient and family understand the high-risk nature of this procedure.
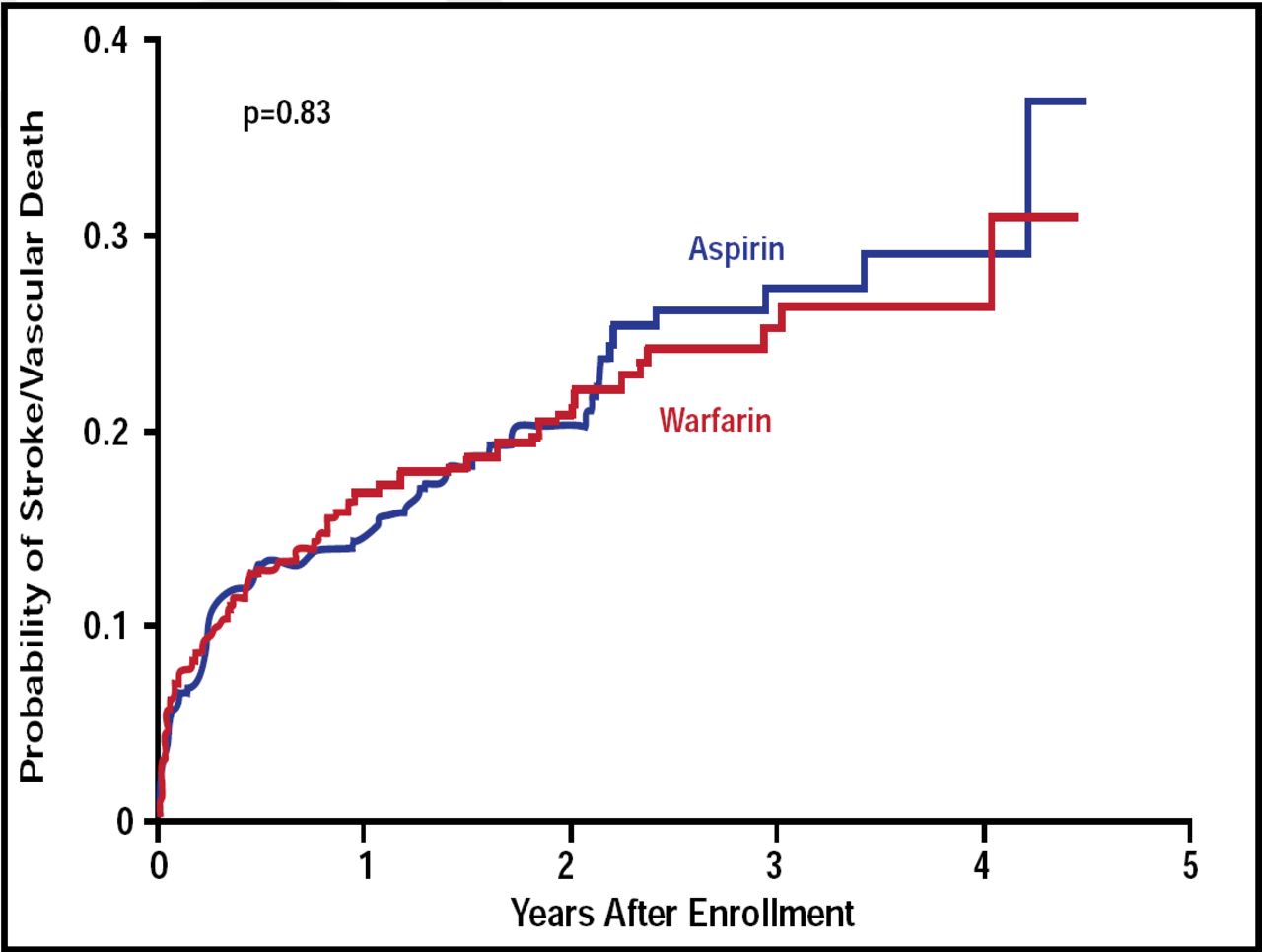
Marc I. Chimowitz, MBChB, Medical University of South Carolina, Charleston, SC, discussed the lessons that were learned from the Warfarin-Aspirin Symptomatic Intracranial Disease (WASID) trial and how the trial impacted the design of the Stenting and Aggressive Medical Management for Preventing Recurrent stroke in Intracranial Stenosis (SAMMPRIS) study.
In the WASID study, warfarin was associated with a high rate of death (9.7% in the warfarin group vs 4.3% in the aspirin group; p=0.02) and major hemorrhage (8.3% in the warfarin group vs 3.2% in the aspirin group; p=0.01). However, the probability of stroke/vascular death (about 22%) at 4.5 years was the same for both warfarin and aspirin (p=0.83; Figure 1) [Chimowitz MI et al. N Engl J Med 2005].

Primary Endpoint: Stroke and Vascular Death.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
It was also noted that elevating blood pressure to protect against hypoperfusion in symptomatic patients with intracranial stenosis is associated with an increased (not decreased, as originally thought) risk of stroke [Chaturvedi S et al. Neurology 2007; Turan TN et al. Circulation 2007]. The WASID study also identified subgroups (patients with stenosis ≥70% after recent symptoms and women) who were at very high risk of stroke in the first year in the territory of the stenotic artery [Kasner SE et al. Circulation 2006].
With these findings in mind, the SAMMPRIS study was designed to compare aggressive medical therapy alone with intracranial stenting (Wingspan stent system) plus aggressive medical therapy in high-risk patients with symptomatic stenosis of a major intracranial artery. The primary endpoint in SAMMPRIS is any stroke or death within 30 days of enrollment or revascularization done during follow-up or stroke in the territory of the stenotic/ stented artery beyond 30 days of enrollment. The mean follow-up is expected to be 2 years. Aggressive medical management includes daily administration of aspirin and clopidogrel for 90 days followed by aspirin alone, blood pressure and low-density lipoprotein reduction, and a lifestyle modification program.
SAMMPRIS enrollment is proceeding well, and the trial is scheduled to be completed in 2013–2014. Regardless of outcome, this study will provide future standard of care for treating intracranial arterial stenosis.
Intracranial stenosis from atherosclerosis accounts for approximately 10% to 15% of all ischemic strokes. Ajay K. Wakhloo, MD, University of Massachusetts, Boston, MA, discussed the challenges of treating intracranial stenosis, starting with early developmental changes of the carotid bulb.
The tortuous morphology that leads to changes in flow dynamics as the carotid bulb develops increases the risk for atherosclerotic plaque and intracranial stenosis later in life [Peterson RE et al. Neurology 1960]. Carotid bulb stenosis is localized and progresses circumferentially from the outer wall toward the carina affecting interstitial flow through the intraepithelial layer (IEL) and in turn affecting shear stress on arterial smooth muscle cells. There is a decrease in shear stress after IEL injury.
Knowledge of cerebral vascular hemodynamics can be used in the assessment of stroke risk and best treatment course for patients with symptomatic vertebrobasilar disease. Using quantitative magnetic resonance angiography to stratify patients on the basis of the presence or absence of distal flow compromise, patients with normal distal flow had an event-free survival (stroke and combined stroke/TIA) of 100% and 96%, respectively. Comparatively, patients with low distal flow experienced a 71% and 53% event-free survival, demonstrating a significantly higher risk of recurrent ischemia (p=0.003). Patients with low flow who subsequently underwent treatment (n=12) had an 82% event-free survival [Amin-Hanjani S et al. Stroke 2005].
Dr. Wakhloo is awaiting results from the Vitesse Intracranial Stent Study for Ischemic Therapy (VISSIT), which is a randomized investigational device exemption (IDE) trial that is comparing medical therapy with stenting for symptomatic stenosis of 70% to 99% of the vessel.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.