

Summary
Clinical outcomes, safety, and recanalization rates using the Merci retriever embolectomy device are similar to those seen in previous prospective studies. In this study, investigators compared data from the Merci Registry with pooled data from the Mechanical Embolus Removal in Cerebral Ischemia [MERCI] and Multi MERCI trials to evaluate the clinical outcomes, safety, and recanalization rates of the Merci retriever embolectomy device in a “real world” setting.
- ischemia
- interventional techniques & devices neurology clinical trials
Clinical outcomes, safety, and recanalization rates using the Merci retriever embolectomy device are similar to those seen in previous prospective studies. In this study by Jovin and colleagues, investigators compared data from the Merci Registry with pooled data from the Mechanical Embolus Removal in Cerebral Ischemia (MERCI) and Multi MERCI trials to evaluate the clinical outcomes, safety, and recanalization rates of the Merci retriever embolectomy device in a “real world” setting.
The primary endpoint was revascularization, defined as Thrombolysis in Cerebral Infarction (TICI) score of 2a or higher. The secondary endpoint was clinical outcomes at 90 days. Outcomes were evaluated at 24 hours (determined by NIH Stroke Score [NIHSS] and symptomatic intracranial hemorrhage [sICH]), discharge (determined by NIHSS and modified Rankin Scores [mRS]), and 90 days (determined by mRS). A total of 625 patients with acute ischemic stroke, large vessel intracranial occlusion, and at least one pass with the Merci retriever were included in the primary analysis. Of the 625 patients, 20% were octogenarians.
While both cohorts who were subjected to comparison presented with severe strokes, patients who were included in the pooled Merci/Multi Merci (M/MM) data had more severe strokes at presentation compared with those in the Merci Registry (mean NIHSS in the Mercy Registry 17.9 versus 19.6 in the M/MM group, p<0.0001). There was no significant difference in comorbidities or occlusion location between the two data sets. The incidence of adjuvant pharmacological thrombolysis (ie, intravenous lytic or intra-arterial lytic) was higher in the Merci Registry than in M/MM (p<0.0001).
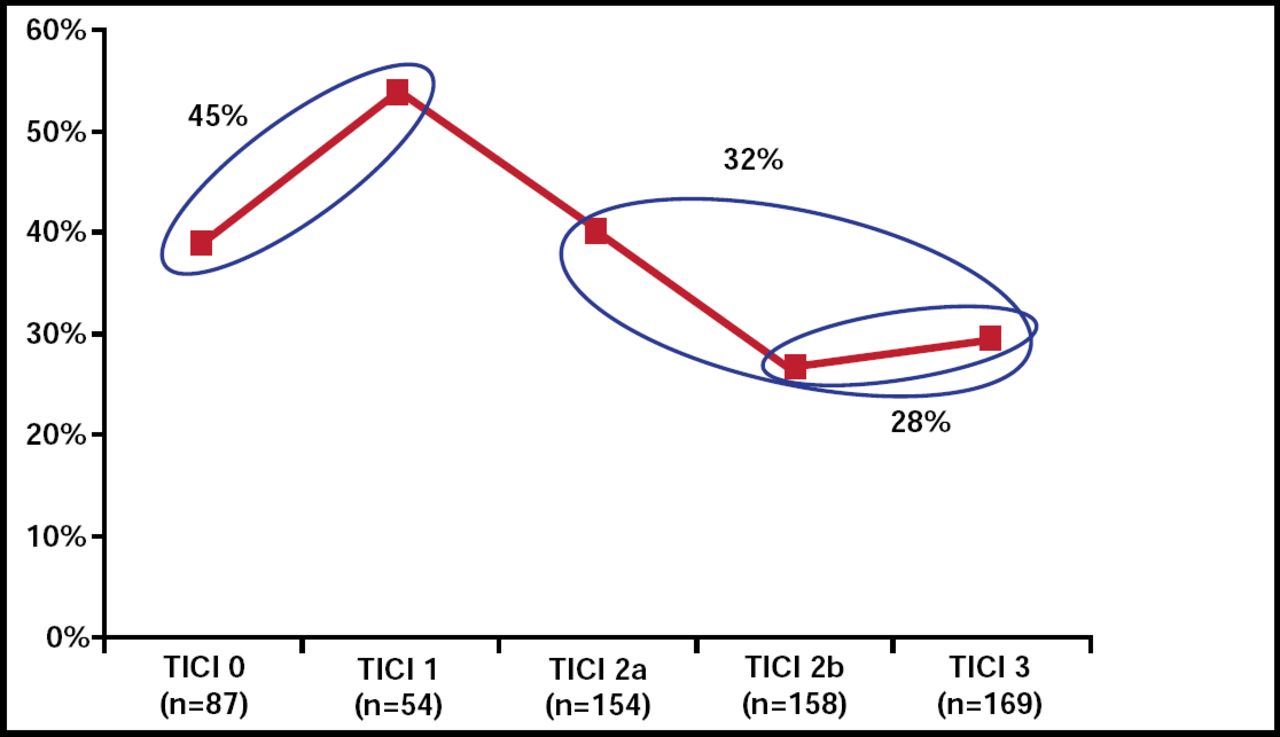
The time from last seen at baseline to procedure onset (in hours) was higher in the Merci registry (5.72±3.28) than in M/MM (4.35±1.76; p<0.001). However, no association was found between time to procedure and clinical outcome. The majority of procedures in the Merci registry occurred between 3 and 8 hours after symptom onset (73.7%). The rate of procedures that started 8 hours or more after symptom onset was higher in the Merci registry (14.1%) than in M/MM (1.3%; p<0.001), highlighting a recent trend toward imaging rather than time-based selection for acute stroke interventions, which, in selected cases, enables expansion of the therapeutic time window beyond 8 hours. Overall, revascularization rates of TICI 2a and TICI 2b-3 were associated with lower mortality rates (32% and 28%, respectively; Figure 1) and with significantly higher rates of favorable clinical outcomes in multivariate analyses (odds ratio 2.97, p< 0.0001)

Mortality Rates According to Revascularization (TICI) Score.
Reproduced with permission from T. Jovin, MD.
Recanalization rates were significantly better in the Merci registry (77%) versus M/MM (65%). However, successful recanalization was defined differently in the two groups, based on TICI score in the Mercy Registry versus TIMI score in the M/MM data. Modified Rankin Scores ≤2 at 90 days and 90-day mortality rates were not significantly different between the two groups. Intubated state during procedure was an adverse predictor of good clinical outcome (p=0.0004) and was associated with a higher risk of mortality (p=0.0141) at 90 days. In a multivariate analysis that looked at revascularized subjects only, baseline NIHSS, age, procedure duration, intubated state during procedures, intra-arterial lytic, and glucose ≥140 mg/dL were significant predictors of clinical outcome at 90 days.
Tudor G. Jovin, MD, Presbyterian University Hospital, Pittsburgh, PA, pointed out two important trends that were identified during this study. First, in support of other multicenter studies that were presented at the International Stroke Conference 2010, intubated state during the procedure was shown to negatively affect clinical outcome throughout this analysis. Second, though time to procedure was not associated with better clinical outcome, procedure duration affected clinical outcome. The shorter the procedure duration, the higher the chance of a good outcome, said Dr. Jovin.
Results of this large, prospective study of mechanical embolectomy with the MERCI device were similar to those found in previous studies with regard to clinical outcome, safety, and recanalization rates. These data confirm that successful recanalization is associated with better clinical outcome. This study also shed some light on the effect of intubation, procedure duration, and time to treatment on clinical outcome. However, this analysis was based on nonrandomized, self-reported data in the absence of a control. Therefore, efficacy of this treatment approach compared with standard medical therapy was not addressed by this study, and further randomized controlled studies are warranted.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.