

Summary
Continuous ultrasound that is delivered by catheter directly into an intracerebral hemorrhage and intraventricular hemorrhage with tissue plasminogen activator for 24 hours appears to be safe and effective for hemorrhage removal. This article discusses findings from the Safety of Lysis with EKOS Ultrasound in the Treatment of Intracerebral and Intraventricular Hemorrhage [SLEUTH] study.
- neurology clinical trials
- interventional techniques & devices
- ischemia
Continuous ultrasound that is delivered by catheter directly into an intracerebral hemorrhage (ICH) and intraventricular hemorrhage (IVH) with tissue plasminogen activator (tPA) for 24 hours appears to be safe and effective for hemorrhage removal. David W. Newell, MD, Swedish Neuroscience Institute, Seattle, WA, presented findings from the Safety of Lysis with EKOS Ultrasound in the Treatment of Intracerebral and Intraventricular Hemorrhage (SLEUTH).
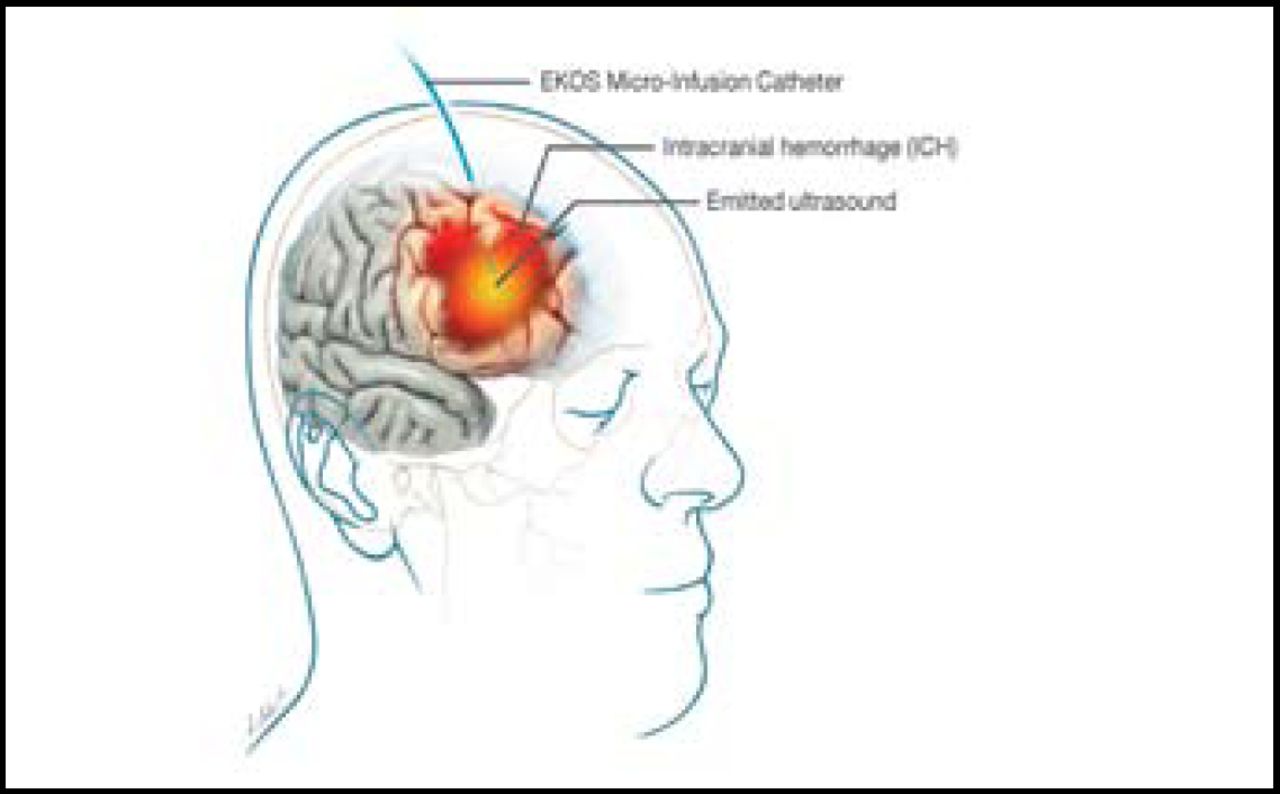
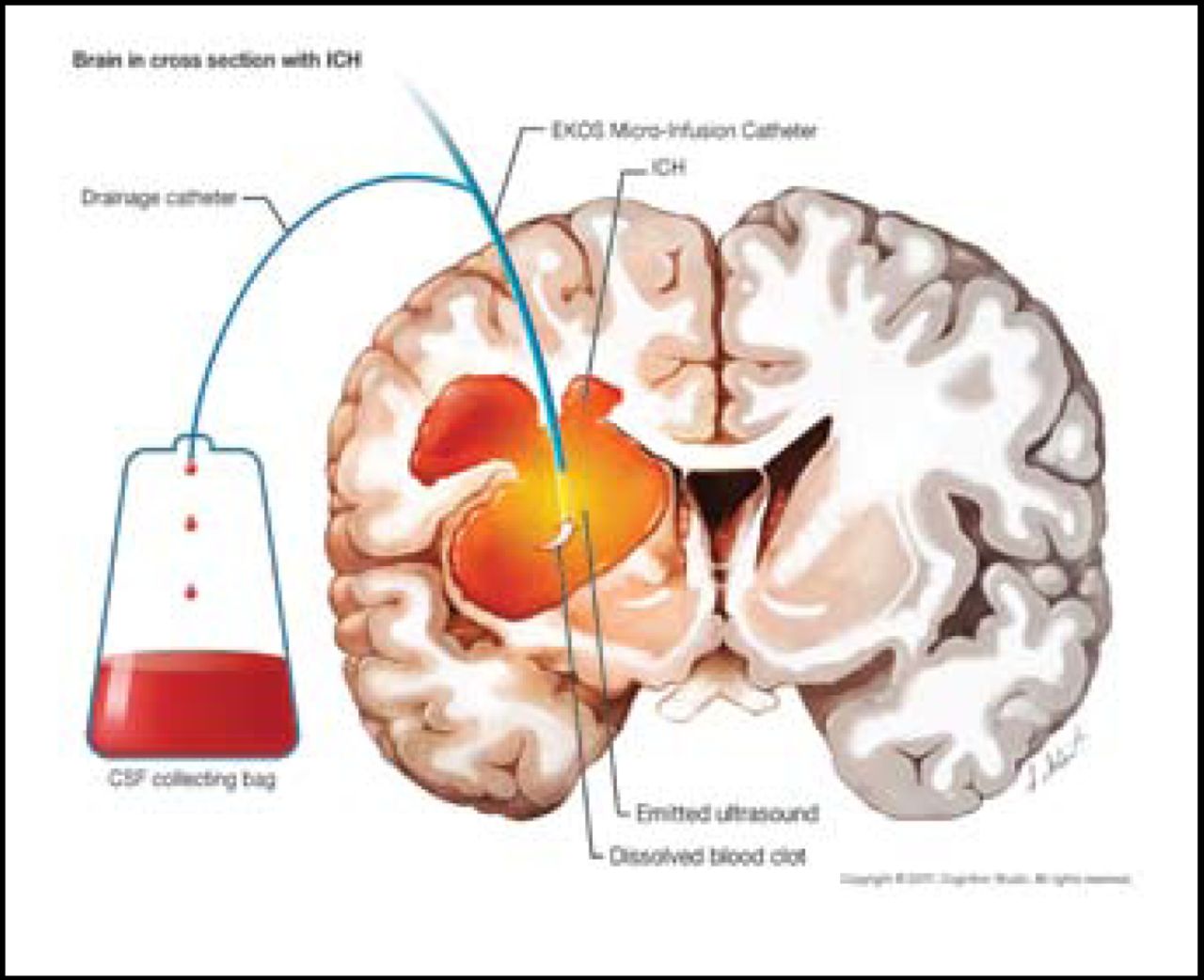
There are many catheter-based treatments for ICH, but clot resolution rates are greatly dependent on proper catheter placement [Morgan T et al. Acta Neurochir Suppl 2008]. Additionally, ultrasound may promote the effect of tPA and aid in the dissolution of clots. The purpose of the SLEUTH study was to evaluate the safety of adding catheter-delivered ultrasound to catheter-based lysis in ICH and IVH (Figures 1A and 1B). This study included 9 patients (mean age=63) who had spontaneous supratentorial ICH ≥25 cc (n=6) and/or IVH (n=3) that obstructed the third and/or fourth ventricles (no documented vascular lesion) with symptom onset <12 hours prior to diagnostic CT scan. Treatment occurred within 72 hours. One ICH patient was subsequently excluded from the study analysis due to catheter breakage that occurred during transport to CT. A neuronavigation system was used to locate the catheter and deliver the lytic, and continuous ultrasound was delivered via catheter for 24 hours. The endpoints were 30-day mortality, symptomatic bleeding rate, brain infection, and blood clot resolution. There was a stopping rule in place for increase in hemorrhage size.

EKOS Micro-Infusion Catheter.
Reproduced with permission from D. Newell, MD.

EKOS Micro-Infusion Catheter.
Reproduced with permission from D. Newell, MD.
One IVH patient died within 30 days of treatment. No other deaths, infections, or rebleeds were observed. There was a 59% ± 5 (SEM) reduction in mean percentage volume after 24 hours of treatment in the ICH group compared with pretreatment stability scans, as determined by CT. A 45.1% ± 13 (SEM) mean percentage volume reduction was observed in the IVH group compared with pretreatment stability scans. Patients who were treated with sonolysis + tPA had faster rates of lysis during the first 24 hours of treatment for IVH (p=0.046) and ICH (p=0.074) compared with similar treatment with tPA alone [Morgan T et al. Acta Neurochir Suppl 2008; courtesy of D. Hanley (unpublished data)].
Dr. Newell concluded that adding catheter-delivered ultrasound to catheter-based lysis appears to be safe and effective for removal of intracerebral or intraventricular hemorrhage. The addition of sonolysis to tPA resulted in increased rates of lysis during the first 24 hours. These encouraging results justify additional clinical trials of catheter drainage of ICH and IVH that employs ultrasound.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.