

Summary
Carotid endarterectomy (CEA) and carotid artery stenting (CAS) are viable options for revascularization, and these strategies are comparable with regard to safety and efficacy for the prevention of ischemic strokes. However, the favorability of CEA and CAS varies according to individual risk factors. This article discusses results from the Carotid Revascularization Endarterectomy versus Stenting [CREST] Trial.
- neurology
- cerebrovascular disease
- ischemia
- interventional techniques & devices
- neurology clinical trials
Details from the CREST Study
Carotid endarterectomy (CEA) and carotid artery stenting (CAS) are viable options for revascularization, and these strategies are comparable with regard to safety and efficacy for the prevention of ischemic strokes. However, the favorability of CEA and CAS varies according to individual risk factors. Wayne M. Clark, MD, Oregon Health Sciences University, Portland, OR, presented results from the long-awaited Carotid Revascularization Endarterectomy versus Stenting Trial (CREST).
CREST was a prospective, multicenter (108 US and 9 Canadian sites), randomized, controlled trial with blinded endpoint adjudication that compared CEA (n=1240) and CAS (n=1262) in patients with symptomatic and asymptomatic stenosis. The primary endpoints were the periprocedural composite of any clinical stroke, myocardial infarction (MI; defined as elevation of cardiac enzymes 2+ times the upper limit of normal plus chest pain or ECG changes with definitive ST changes), and death and postprocedural ipsilateral stroke in the treated vessel for up to 4 years. Secondary endpoints were differential efficacy by symptomatic status, gender and age, differential restenosis, and quality of life and cost effectiveness [CREST. Int J Stroke 2010].
Stroke was defined as an acute neurological ischemic event of ≥24 hours in duration with focal signs and symptoms that were adjudicated by at least 2 neurologists who were blinded to treatment. Symptomatic and asymptomatic carotid stenosis was determined by angiography, ultrasonography, or CTA/MRA. Patients with chronic atrial fibrillation, evolving stroke or major stroke that was likely to confound study endpoints, MI within 30 days, unstable angina, or enzyme-only MI were excluded from study participation. Baseline characteristics were well matched. Most participants had a high degree of stenosis (>70% stenosis in 85% of CAS patients and 87% of CEA patients), and procedures were performed an average of 20 to 25 days after the qualifying event in symptomatic patients.
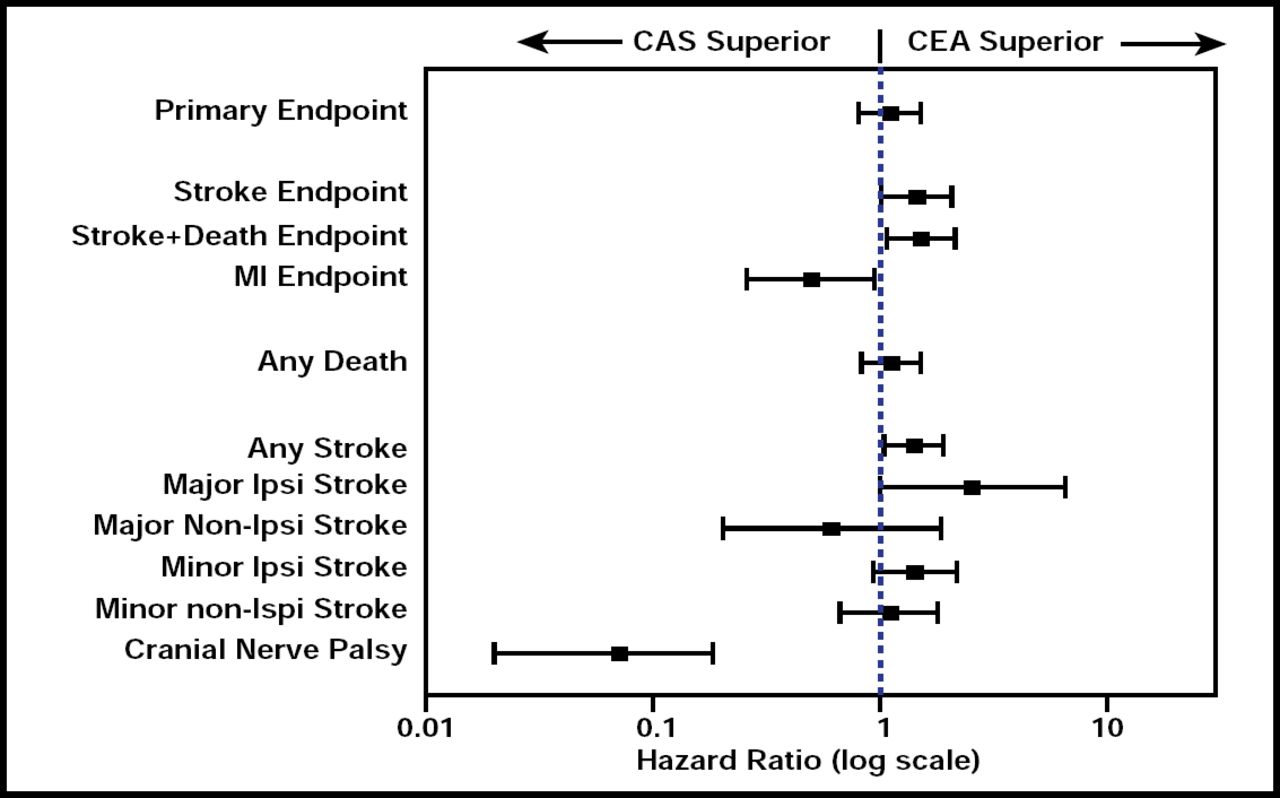
No significant differences were found in the primary endpoints, and no differences between the two procedures were observed that were related to symptomatic status or gender. However, CAS was superior to CEA in patients aged ≤70 years, while more favorable outcomes were noted with CEA in patients aged >70 years (p interaction=0.020). Overall, there was no difference in outcome when looking at the periprocedural composite of all stroke and MI, but when considering these risks individually, the differences were statistically significant. CEA was associated with lower rates of all stroke (HR, 1.79; 95% CI, 1.14 to 2.82; p=0.01), and CAS was associated with lower rates of MI (HR, 0.50; 95% CI, 0.26 to 0.94; p=0.03; Figure 1). Periprocedural cranial nerve palsies were more frequent in patients who received CEA than CAS (p<0.0001). Quality of life and cost effectiveness data from CREST are pending.

CEA/CAS Comparison.
Reproduced with permission from W. Clark, MD.
“At experienced centers, both CEA and CAS appear to have low perioperative complications and excellent long-term results. I feel that we now have two options we can offer to our patients to prevent carotid artery strokes,” Dr. Clark said.
Thomas G. Brott, MD, Mayo Clinic, Jacksonville, FL, an investigator in the CREST trial, elaborated on these findings. The average life expectancy has also increased in recent years. Therefore, the age-related data that were gleaned from CREST are quite important. Dr. Brott pointed out that comparing CEA and CAS in both asymptomatic and symptomatic stenosis was a key feature of CREST, as it allowed the results to be applied to a more general population. Previous studies have focused on more specific symptom-driven cohorts. CTA and MRA were added during the latter part of the study to ensure that the documented stenosis was genuine. CREST attempted to accommodate changes in technology as the study progressed (eg, the addition of CTA/MRA).
The procedures seem to be clinically durable. “One explanation for this durability may be that modern medical therapy may have progressed to the point where perhaps the procedure did not necessarily have to be done,” said Dr. Brott. Medical therapy has advanced dramatically over the past decade, and the possibility that successful outcomes are owing more to better medications than to the procedures themselves merits further investigation.
How does CREST Compare with Other Trials?
Martin Brown, MD, University College, London, UK, discussed some other randomized controlled trials (RCTs) in relation to CREST and CEA versus CAS. “RCTs provide the best data to assess the effects of treatment and, more importantly, assure that patients are well matched. However, an RCT is only as good as its sample size,” said Dr. Brown. While CREST results correspond with previous CEA and CAS study findings, there is a huge disparity between sample sizes for these studies.
In the SPACE study, 30-day safety data favored CEA over CAS (rate of stroke or death 6.5% for CEA vs 7.7% for CAS). However, this study was not very large and was discontinued due to futility and funding issues. There were several crucial differences in SPACE compared with CREST. For example, MI was not included as an outcome event, and there were a variety of stents and devices that were approved in SPACE. The rate of ipsilateral stroke or death was identical for CEA and CAS (5.9%) in patients aged younger than 76 years in SPACE but favored CEA (7.5% vs 11.1% for CAS) in patients aged older than 76 years [The SPACE Collaborative Group. Lancet 2006].
The EVA-3S study demonstrated results that were similar to those found in the CREST study. EVA-3S was discontinued early (after randomization of 527 patients) due to significantly better 30-day outcomes for CEA compared with CAS. The rate of stroke or death was significantly lower for CEA compared with stenting (3.9% vs 9.6% for CAS; p=0.01) [Mas JL et al. N Engl J Med 2006].
The International Carotid Stenting Study (ICSS) was similar to CREST by design, and it was thought that the results would correlate. One major difference in ICSS is that it included only patients with recently symptomatic carotid stenosis. The use of protective devices and the type of stent were left to the interventionalists' discretion, as was the use of aspirin and clopidogrel prior to stenting. At 120 days, the primary short-term outcome (stroke, death, or periprocedure MI) favored CEA (p=0.006). Thirty-day rates of stroke or death were higher in the CAS group compared with CEA (p<0.001) [International Carotid Stenting Study Investigators. Lancet 2010].
In a substudy of ICSS that focused on MRI detection of new ischemia, the rates of new ischemia in the CEA group were lower than in the CAS group (OR 5.21; 95% CI, 2.78 to 9.79; p<0.0001) [Bonati et al. Lancet Neurol 2010]. Silent infarcts were more frequent after CAS, regardless of age, and were more common when protection devices were utilized.
A subgroup analysis of pooled data from EVA-3S, SPACE, and ICSS is currently underway. Preliminary data have demonstrated favorable outcomes within 30 days of treatment for CEA versus CAS, particularly in regard to the risk of any stroke or death (p<0.0001) [data not yet published]. However, more data are needed to determine the long-term efficacy of CEA and CAS, and it is not yet known if the benefit is equivalent.
Who Benefits from Treatment?
Peter Rothwell, MD, University of Oxford, Oxford, UK, showed that neither treatment is merited in many patients, and these interventions should only be used in those patients with severe symptomatic stenosis. Although some of the excess stroke risk that is associated with CAS versus CEA is due to minor stroke, these events should be taken very seriously, because it is a reduction in minor stroke that accounts for most of the benefit of these interventions compared with medical treatment alone in the first place, said Dr. Rothwell. In symptomatic patients, the procedural risk of stroke with CAS in CREST was double that of CEA (6% vs 3%), which is consistent with previous studies. Based on these findings, CAS may be no better than medical treatment alone in moderately symptomatic patients. The similar relative excess risk of stroke with CAS versus CEA in patients with asymptomatic stenosis will also result in better outcomes on intensive medical treatment alone in this group [Rothwell PM. Lancet 2010].
Therefore, who will benefit most from CEA or CAS? The answer to that question is not as straightforward as one would hope. Men have shown a greater benefit from CEA than women [Rothwell PM et al. Lancet 2004]. However, benefit and risk increase with age independently of gender [Rothwell PM et al. Lancet 2005]. The increased procedural risk of stroke with CAS versus CEA in patients aged over 65–70 years appears to be consistent across multiple studies and may be due to the increase in calcification of vessels and plaques with age [Redgrave J et al. Stroke 2010. In press]. These and other risk factors should be weighed carefully before deciding on a treatment strategy.
Results from the CREST study have elucidated the benefit and risk of CEA versus CAS, particularly in relation to individual outcomes, such as MI and stroke. While the risk of stenting may have been expected to decrease over time in light of technological advances and more procedural experience, this has yet to be shown to be the case. More data are needed to assess the long-term risks of CAS. Given the current evidence of a greater procedural risk of stroke, greater asymptomatic infarction, and greater restenosis with CAS versus CEA, CEA must remain the treatment of choice in routine clinical practice.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.