

Summary
Diabetes mellitus (DM) adds a layer of complexity to cardiovascular disease (CVD), and mortality rates among individuals with DM are 2- to 3-fold higher compared with those without DM [Preis SR. Circulation 2009]. This article discusses the challenges and treatment strategies that are associated with DM and CVD.
- cardiometabolic disorder
- coronary artery disease
- diabetes mellitus
Diabetes mellitus (DM) adds a layer of complexity to cardiovascular disease (CVD), and mortality rates among individuals with DM are 2- to 3-fold higher compared with those without DM [Preis SR. Circulation 2009]. Richard Nesto, MD, FACC, Lahey Clinic Medical Center, Burlington, MA, discussed the challenges and treatment strategies that are associated with DM and CVD.
Recent studies have investigated the effect of stringent glucose regulation on CVD risk in patients with type 2 DM. In the Action to Control CardiOvascular Risk in Diabetes (ACCORD) study, 10,251 patients with a median glycated hemoglobin A1c (HbA1c) level of 8.1% were randomized to receive either intensive (target HbA1c <6.0%) or standard (target HbA1c 7.0% to 7.9%) therapy. The primary outcome was a composite of nonfatal myocardial infarction (MI), nonfatal stroke, or death from cardiovascular (CV) causes (Table 1). Intensive therapy was discontinued after a mean follow-up of 3.5 years due to increased rates of mortality in this group (HR, 1.22; 95% CI, 1.01 to 1.46; p=0.04). Dr. Nesto pointed out that the excess risk of death that was associated with intensive treatment occurred in patients who demonstrated no HbA1c reduction from baseline in the first year and/or had an average HbA1c level of >7.0%. Hypoglycemia was also more frequent in the intensive therapy group (p<0.001); however, there was no evidence that it contributed to increased mortality [ACCORD Study Group. N Engl J Med 2008].
ACCORD Primary and Secondary Outcomes.*
Findings from the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) study demonstrated that intensive glucose control (use of modified release gliclazide plus other drugs to achieve HbA1c levels ≤6.5%) reduced the incidence of combined major macrovascular and microvascular events, as well as microvascular events alone, compared with standard therapy at 5 years (p=0.01 for both), primarily owing to a 21% reduction in relative risk of nephropathy (HR, 0.79; 95% CI, 0.66 to 0.93; p=0.006) [The ADVANCE Collaborative Group. N Engl J Med 2008]. Findings from the United Kingdom Prospective Diabetes Study (UKPDS), a prospective study of intensive glucose lowering in patients with type 2 DM, further support the microvascular benefit of intensive glucose control. In UKPDS, patients with type 2 DM were randomized to either conventional therapy (dietary restriction) or intensive therapy (either sulfonylurea or insulin, or metformin in overweight patients). Subjects who received intensive glucose therapy had a lower risk of microvascular complications compared with those who received conventional therapy [Holman RR. N Engl J Med 2008]. A 10-year follow-up revealed continued reductions in the relative risk of microvascular disease (24%; p=0.001) as well as risk reductions for MI (15%; p=0.01) and death from any cause (13%; p=0.007) in the sulfonylurea/insulin group, which emerged over time as more events occurred. Significant reductions in the relative risk of MI (33%; p=0.005), any diabetes-related endpoint (21%; p=0.01), and death from any cause (27%; p=0.002) were noted in the metformin group compared with standard therapy at the 10-year post-trial follow-up.
Robert L. Frye, MD, Mayo Clinic, Rochester, MN, discussed the Bypass Angioplasty Revascularization 2 Diabetes (BARI-2D) study, which evaluated treatment options for coronary artery disease (CAD) and glycemic control in patients with type 2 DM. Dr. Frye emphasized that BARI-2D is a comparison of management strategies for myocardial ischemia and glycemic control rather than a test of individual diabetes drugs, different HbA1c targets, or percutaneous coronary intervention (PCI) versus coronary artery bypass grafting (CABG). In BARI-2D, 2368 patients with type 2 DM (mean duration of 10.4 years and mean HbA1c=7.7%) and documented myocardial ischemia (≥1 significant coronary stenosis at angiography) were randomized as part of a 2-by-2 factorial design to receive either prompt revascularization (PCI or CABG, as determined by the local cardiologist) with intensive medical therapy or intensive medical therapy alone and subsequently randomized to either insulin sensitization (IS) or insulin provision (IP) therapy. The primary endpoints were the rate of death and a composite of death, MI, or stroke (major CV events).
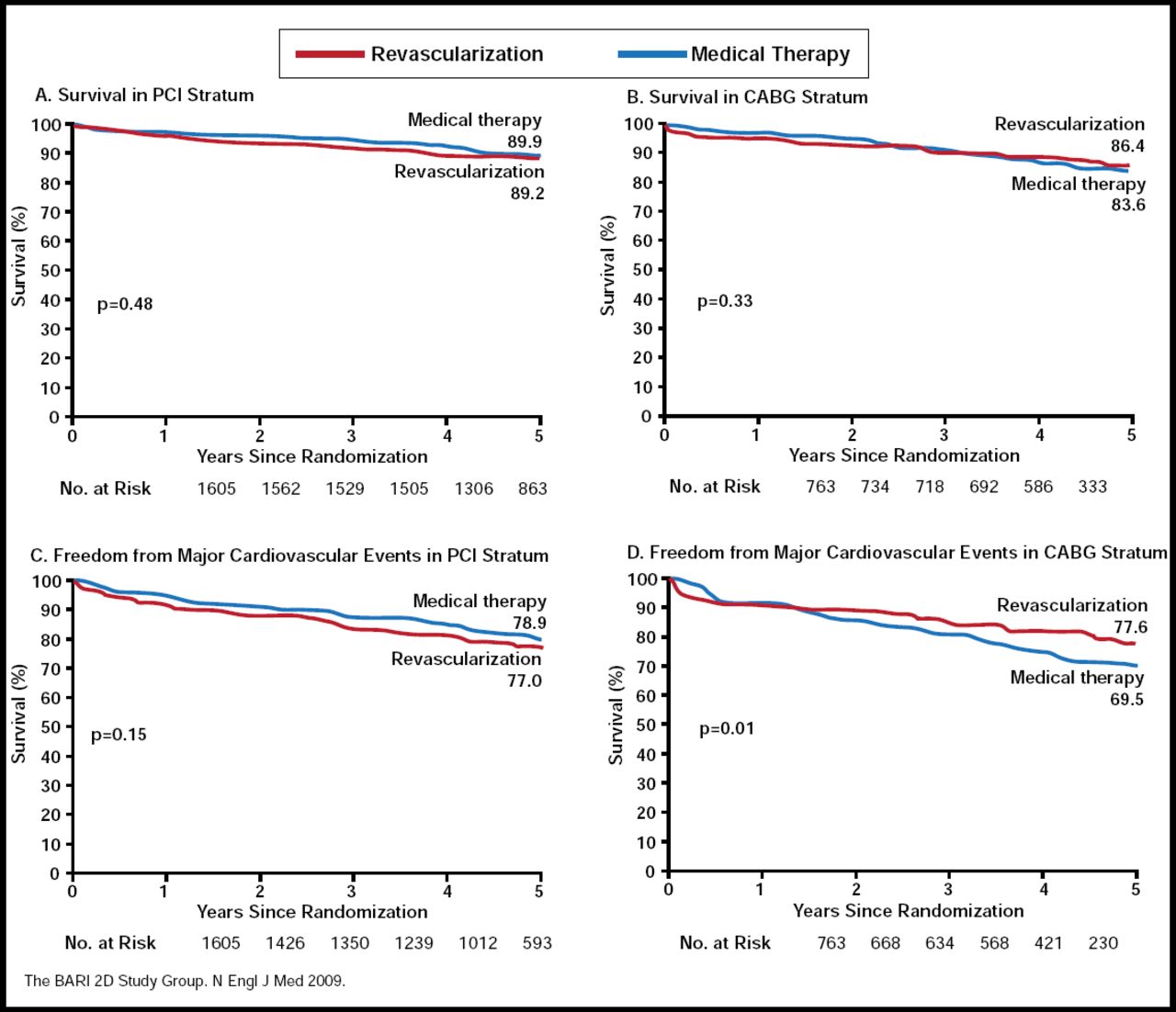
Overall, CV events and mortality were similar for prompt revascularization versus delayed or no revascularization (p=0.70 for CV events and p=0.97 for survival), as well as for IS versus IP (p=0.13 for CV events and p=0.89 for survival) at 5 years. However, among patients who were selected for the CABG stratum, revascularization was associated with a lower rate of major CV events compared with medical therapy (p=0.01), particularly among those who received IS (p=0.002; Figure 1). Additionally, IS therapy was associated with less weight gain (0.3 vs 2.1 kg), decreased waist circumference (−0.1±9.1 cm vs +1.9±8.4), and fewer hypoglycemic events (5.9% vs 9.2%; p=0.003) compared with IP therapy [The BARI-2D Study Group. New Engl J Med 2009; Rutter MK & Nesto RW. Diab Vasc Dis Res 2010]. Dr. Frye concluded that for patients who are similar to those in BARI 2D with extensive multivessel disease, CABG has an advantage in reducing event rates compared with initial medical therapy alone. In applying these results in clinical practice, comorbidities, age, and other factors must also be considered. The role of insulin sensitization merits further investigation, based on the BARI-2D results, added Dr. Frye.

BARI-2D: Rates of Survival and Freedom from Major CV Events, According to PCI and CABG Strata.
Copyright © 2009 Massachusetts Medical Society. All rights reserved.
Metabolic Syndrome (MetS) also plays a role in CVD risk and may predict diabetes independently of other factors [Lorenzo C. Diabetes Care 2003]; therefore, “diabeteslike” strategies for prevention are merited, noted Dr. Nesto. MetS components include obesity, increased waist circumference, fasting glucose >100 mg/dL, high triglyceride/HDL ratio, microalbuminuria, and C-reactive protein >3.0. MetS has been associated with lipid-rich plaques, which may contribute to increased risk of plaque vulnerability [Amano T. J Am Coll Cardiol 2007]. There is also a strong association between abnormal glucose metabolism, a characteristic of MetS, and mortality, and there may be indications of MetS and CVD risk early in life [Barr EL. Circulation 2007; Caballero AE. Diabetes Care 2008; Atabek ME. PediatrRed 2007; Urbina Em. Circulation 2009]. Delivering optimal “global” treatment is a responsibility that must be shared by all health care providers, concluded Dr. Nesto.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.