

Summary
Over the last 20 years, the use of mechanical valves for valve replacement has fallen out of favor. While the decline has been due primarily to a high incidence of thromboembolism and the risk of hemorrhage that is associated with the anticoagulants that are used to prevent thrombosis, continuous improvements in both the Ross Procedure and valvular prosthesis processing have also been factors in the drop in use of mechanical valves. This article discusses advances in both valves and implantation procedures.
- valvular disease
Over the last 20 years, the use of mechanical valves for valve replacement has fallen out of favor. While the decline has been due primarily to a high incidence of thromboembolism and the risk of hemorrhage that is associated with the anticoagulants that are used to prevent thrombosis, continuous improvements in both the Ross Procedure and valvular prosthesis processing have also been factors in the drop in use of mechanical valves, said Alain Carpentier, MD, Hôpital Européen Georges Pompidou, Paris, France.
Data from 267 consecutive patients (mean age 33.8 years; range 18 to 50 years) who underwent the Ross Procedure, performed at the Cardiologic Hospital in Lille, France, yielded an early mortality rate of 1.9% and a late mortality rate of 5.8% over an 18-year period, mostly unrelated to cardiac issues. Advantages of the Ross Procedure include the absence of thrombogenicity and hemolysis, resistance to infection, and growth potential; disadvantages include technical complexity, the potential for trading one-valve disease for two-valve disease, and unknown long-term durability. A weakness of the procedure is the number of reoperations on the autograft and/or the homograft. Patient selection is crucial to a positive outcome. Absolute contraindications for the Ross Procedure include Marfan syndrome, connective tissue disorders, aortic valve regurgitation (AR), and an abnormal pulmonary valve. Relative contraindications include LV function <30%, aortic annulus >35 mm, multivessel coronary artery disease, and history of mediastinal radiotherapy.
Advances in bioprostheses include improved preservation and stent design; larger, more flexible stents; and the use of glutaraldehyde-treated bioprostheses to mitigate calcification, which was often a problem with earlier devices [Carpentier SM et al. Ann Thorac Surg 1998].
Given the morbidity and mortality that are associated with cardiac surgery, there is growing interest in transcatheter valve implantation. John Webb, MD, St Paul's Hospital, University of British Columbia, Vancouver, Canada, discussed the advances in both valves and implantation procedures.
Since 2005, there have been more than 15,000 transcatheter aortic implantations. The two most commonly used valves are the Edwards SAPIEN and the CORE valve. Both have excellent hemodynamics and undergo rigorous testing, similar to that used for surgical valves, and no structural failure has been reported to date for either valve. Delivery systems are also improving from the balloon catheter to a special delivery catheter with nose cones. Aortic sheaths, which started at 24 French (F), are now at 18 F and are expected to be at 16 F or 14 F within a few years. Increasingly sophisticated screening has helped to reduce femoral complications by assisting in identifying patients who are better suited for a transapical or subclavian implantation.
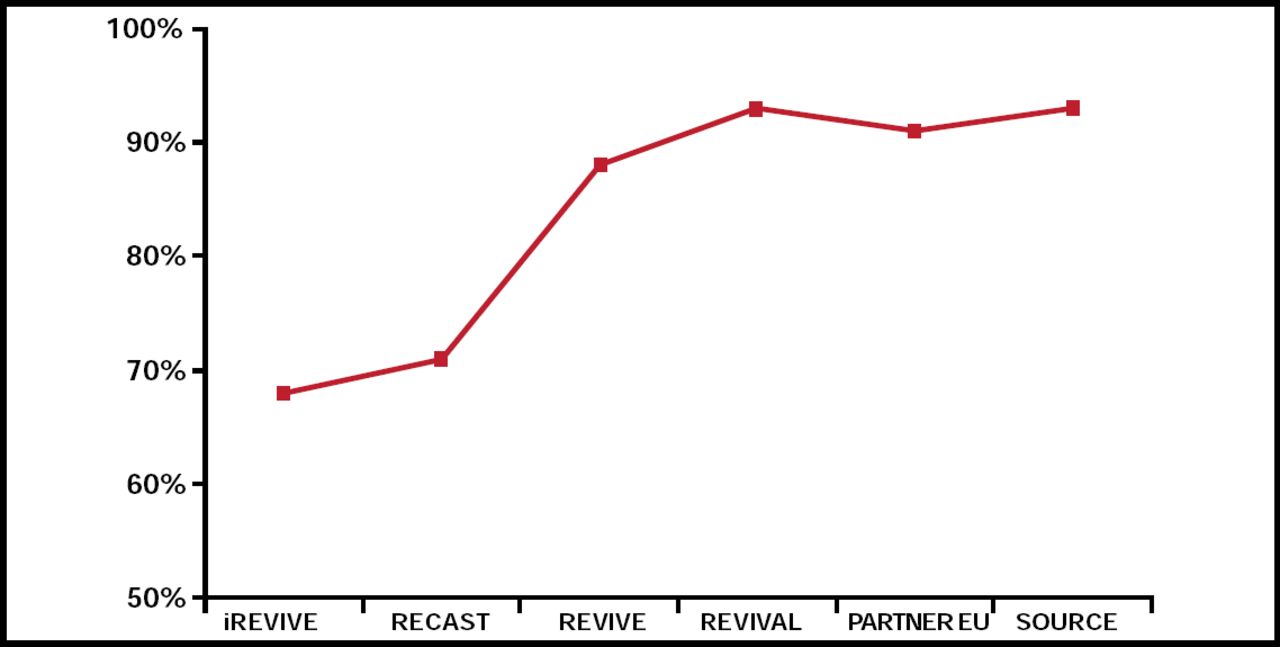
Recent data from the Vancouver High-Risk Percutaneous Registry show a 30-day mortality rate of 4.9% with transaortic valve replacement. Around the world, the survival rate in SAPIEN transarterial trials continues to improve and is now well over 90% (Figure 1). The incidence of stroke is very low (2% to 3%) and is comparable with surgery in high-risk patients. Data from matched registries indicate that ejection fraction (EF) improves more in patients who undergo transcatheter replacement compared with traditional surgical approaches and that rates of renal failure are lower. Data are anxiously awaited from the PARTNER (Placement of AoRTic TraNscathetER) Trial [NCT00530894], which will compare the safety and efficacy of the Edwards SAPIEN valve, delivered transfemorally or transapically, in high-risk symptomatic patients with severe aortic stenosis. The study is currently recruiting and is expected to complete in 2014.

SAPIEN Transarterial Trials Demonstrating Improving Outcomes (30-Day Survival).
Blase A. Carabello, MD, Baylor College of Medicine, Houston, TX, discussed surgery for patients with aortic regurgitation (AR) or mitral regurgitation (MR). Noting that these two conditions were often lumped together as volume-overloading lesions, Dr. Carabello stressed that they have different pathophysiologies. While end diastolic stress is increased in both types of patients, only patients with AR show increased systolic stress, which can be as high as that seen with aortic stenosis. Understanding this distinction helps to explain what happens when the valve is repaired. Because these patients have very high afterload, corrective surgery results in a drop in systolic pressure, a decrease in the radius of the ventricle, and diminished wall stress. These factors lead to an improvement in EF [Chaliki HP et al. Circulation 2002]—which distinguishes surgical correction of AR compared with MR.
Dr. Carabello used two case studies to discuss the important factors to consider when establishing a treatment plan for a patient with AR. In an asymptomatic 45-year-old man with severe AR, left ventricular (LV) end systolic diameter (ESD) of 4.0 cm, and LV end diastolic diameter (EDD) of 6.5 cm, Dr. Carabello said he saw no need to rush this patient into surgery, because there was only a 4% annual risk of developing symptoms or going on to asymptomatic LV dysfunction. He suggested annual follow-up with surgery only if the patient develops symptoms, the EF approaches 55%, or the ESD approaches 5.0 cm. Alternatively, when presented with a 52-year-old male with class III symptoms, severe AR, EDD 8.2 cm, ESD 7.4 cm, and EF=20%, Dr. Carabello said he would treat with ACE inhibitors and diuretics and reevaluate in 3 months. In the absence of improvement Dr. Carabello would proceed to surgery. The key differences between these two patients are the presence of symptoms, marked dilation of the LV in systole, and decreased LV function, any one of which may be a reason to consider aortic valve surgery.
Asymptomatic patients with severe degenerative MR can be safely followed up until either symptoms occur or currently recommended cutoff values for LV size, LV function, or pulmonary arterial hypertension are reached. In one study, patients with severe MR were followed with a watchful waiting strategy for a mean of 62±26 months. Survival that was free of any indication for surgery was 92±2% at 2 years, 78±4% at 4 years, 65±5% at 6 years, and 55±6% at 8 years [Rosenhek R et al. Circulation 2006]. However, MR is not well tolerated for long. Dr. Carabello said that “…letting the patient become very symptomatic is the wrong thing to do.” In fact, a case can be made for considering surgery early in patients with severe MR, even in the absence of severe symptoms, to avoid LV dysfunction.
Reflective of this data, the guidelines for MR have been moved from 2b to 2a for patients with no symptoms and preserved LV function (EF>0.60, ESD<40 mm) and in whom repair is likely. On average in the United States, 57% of valves are repaired. Data regarding mitral repair show that there is substantial reverse remodeling and improvement in quality of life but no mortality benefit.
Ted E. Feldman, MD, Evanston Hospital, Evanston, IL, provided a glimpse into the future of MR repair. In one study of Endovascular Edge-to-Edge (E2E) valve repair for MR, a retrospective analysis of clinical and echocardiographic data showed results that were similar to conventional repair with annuloplasty. After 5 years, 90±5% of patients (n=29, mean age 63.8 years, 45% NYHA class III) were free from the combined endpoint of recurrent MR that was more severe than grade 2 and reoperation [Maisano F et al. Euro Intervention 2006]. Mitral valve repair also has been performed using a surgically created double orifice. Percutaneous repair that is based on this surgical approach has been developed using the Evalve MitraClip device to secure the mitral leaflets. Percutaneous repair with the MitraClip system can be accomplished with low rates of morbidity and mortality, with acute MR reduction to <2+ in the majority of patients, and with sustained freedom from death, surgery, or recurrent MR in a substantial proportion of patients. Kaplan-Meier freedom from death was 95.9%, 94.0%, and 90.1% and freedom from surgery was 88.5%, 83.2%, and 76.3% at 1, 2, and 3 years, respectively [Feldman T et al. J Am Col Cardiol 2009].
New devices that are now used in the coronary sinus approach include the Edwards MONARC, the Cardiac Dimensions CARILLON, and Viacor's Shape-Changing Rods. Development of these devices has been limited because most patients realize only a one-grade reduction in MR, and more importantly, the devices have been associated with circumflex artery compression or ischemia, which, in some patients, has been associated with MI. The likelihood that these devices will only be appropriate for a select group of patients has prompted the development of new devices for the direct approach to the mitral annulus. Other approaches for MR repair include combining procedures, such as CRT + Mitral Valve Clip or mitral valve annuloplasty + E2E repair. Additional novel approaches that are under development include premeasured artificial chordate for mitral repair [Gillinov AM & Banbury MK Ann Thorac Surg 2007] and percutaneous mitral valve replacement.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.