

Summary
Persons with psychiatric disorders often have a myriad of comorbid medical conditions that can add to risk for premature morbidity and mortality. Important conditions that increase risk for cardiovascular disease and diabetes include overweightness and obesity, dyslipidemia, hypertension, hyperglycemia, and smoking, all often interrelated by insulin resistance.
- Schizophrenia
- Psychopharmacology
- Cardiometabolic Disorder
- Lipid Disorders Clinical Trials
Persons with psychiatric disorders often have a myriad of comorbid medical conditions that can add to risk for premature morbidity and mortality. Important conditions that increase risk for cardiovascular disease and diabetes include overweightness and obesity, dyslipidemia, hypertension, hyperglycemia, and smoking, all often interrelated by insulin resistance. The public health construct called the metabolic syndrome is defined by specific criteria for waist circumference, fasting plasma triglyceride, glucose and high-density lipoprotein (HDL) cholesterol, and blood pressure, while the insulin resistance syndrome more broadly includes a range of insulin resistance-associated changes in glucose, uric acid, and lipid metabolism, as well as proinflammatory and prothrombotic changes. Important modifiable risk factors for insulin resistance and these associated changes include increased body adiposity (particularly central or truncal) and reduced fitness, common conditions in individuals with major mental illness.
The metabolic syndrome is prevalent among patients with major depressive disorder (MDD), bipolar disorder (BD), and schizophrenia, and it can lead to increases in treatment cost, morbidity, and mortality. Concerns about the association between antipsychotic treatment and metabolic risk have been raised by increasing numbers of reports that have described diabetes, hyperglycemia, and lipid dysregulation in patients who have been treated with some second-generation (or atypical) antipsychotics, as well as some first-generation agents [Newcomer JW. CNS Drugs 2005].
Manuel Arrojo-Romero, MD, Complejo Hospitalario Universitario, Santiago de Compostela, Spain, presented data that showed that the metabolic syndrome and glucose disturbances are highly prevalent among elderly persons (mean age 70 years) who are diagnosed with schizophrenia. In a sample of elderly chronic schizophrenic inpatients (n=82), 54.9% were diagnosed with the metabolic syndrome, 26.8% with diabetes, 58.5% with hyperglycemia, and 8.5% with hyperinsulinemia. A significant association (p<0.01) was found between insulin resistance and body mass index (BMI) (r=0.37), waist circumference (r=0.37), triglyceride levels (r=0.51), and low levels of high-density lipoprotein (HDL) cholesterol (r=0.26; p<0.05). The majority of the patients (79%) were being treated with 2 or more antipsychotics.
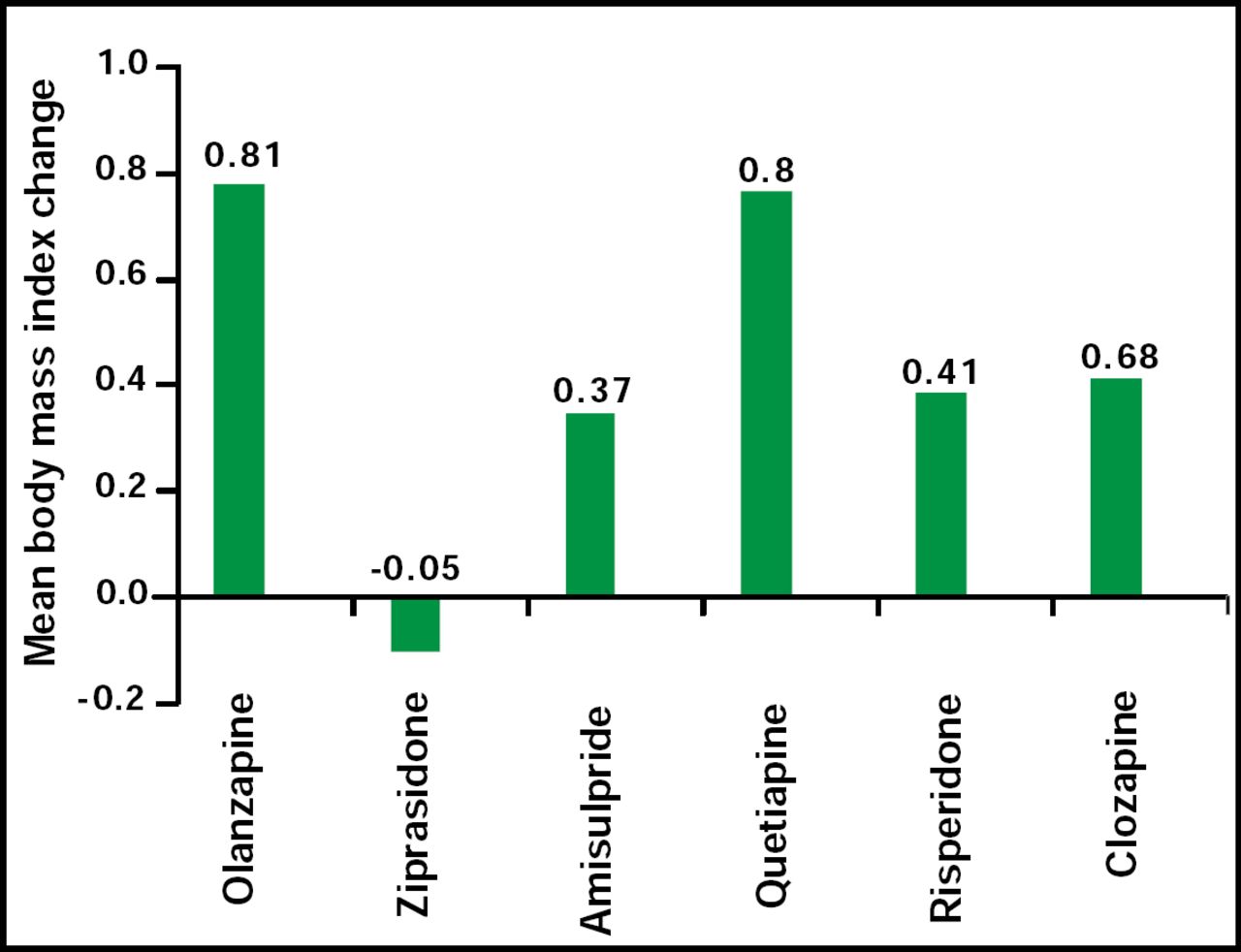
Similar results were reported in a younger population (mean age 45 years) of schizophrenia patients. Hans Rittmannsberger, MD, Landesnervenklinik Wagner-Jauregg, Department of Psychiatry, Linz, Austria, assessed body weight, HDL, low-density lipoprotein cholesterol (LDL), total cholesterol, triglycerides, and fasting glucose in 398 patients who were admitted for inpatient psychiatric treatment at admission and discharge (average stay=24 days). In general, serum lipids worsened by the time of discharge. Patients gained an average of 0.8 kg, while the BMI increased by an average of 0.3 kg/m2 (Figure 1). Fasting glucose improved, decreasing a mean of 3.9 mg/dL. All second-generation antipsychotics were associated with a worsening of lipid values, wherein risperidone showed the least effect. Fasting glucose improved with all drugs except clozapine. All drugs were associated with weight gain except ziprasidone. Olanzapine and quetiapine appeared to have the greatest negative impact on parameters of the metabolic syndrome.

Mean BMI Change.
Susanne Kraemer, Lilly Deutschland, GmbH, Germany, presented data that examined the relationship between the metabolic syndrome and antipsychotic treatment in patients with schizophrenia. Patients (n=476) were treated with olanzapine, risperidone, quetiapine, atypical and typical antipsychotics, or combination therapy. Abnormal values for abdominal obesity, triglycerides, HDL, blood pressure, and fasting glucose, as established by the National Cholesterol Education Program and the American Heart Association, were the defining criteria for the metabolic syndrome. The risk factor of high blood triglycerides had the highest concordance with the metabolic syndrome, whereas the remaining risk factors had a medium concordance. Patients who received typical (first-generation) antipsychotic medications had a higher prevalence of the metabolic syndrome than those who received olanzapine and risperidone (second-generation).
René S. Kahn, MD, University Centre Utrecht, Utrecht, The Netherlands, used data from EUFEST (European First Episode Schizophrenia Trial) to compare the long-term effects of first- and second-generation antipsychotics on the metabolic syndrome and coronary heart disease risk factors. The first-generation antipsychotic haloperiodol was compared with the second-generation antipsychotics amisulpride, olanzapine, quetiapine, and ziprasidone. There were differences in metabolic side effects and cardiovascular risks between first- and second-generation antipsychotics in schizophrenia patients. Ziprasidone-treated patients had significantly (p<0.05) smaller increases in waist circumference compared with haloperiodol patients. Median percentage changes in triglyceride and HDL levels were 34% and −12% for amisulpride, 7% and 0% for haloperiodol, 9% and −9% for olanzapine, 11% and 5% for quetiapine, and −31% and −3% for ziprasidone, respectively. Haloperidol use was also associated with higher rates of smoking compared with second-generation antipsychotics.
The increasing use of antipsychotics in children to modulate irritability and aggressive behavior in the context of a national epidemic of childhood obesity increases the risk of adverse metabolic changes in these children. The Metabolic Effects of Antipsychotics in Children (MEAC) study, an NIH-funded project that was conducted at Washington University in St. Louis under the direction of John Newcomer, MD, evaluated antipsychotic-naïve children (aged 6 to 18 years) with behavioral problems who were randomly assigned to 12 weeks of treatment with the second-generation antipsychotics olanzapine, risperidone, and aripiprazole. The MEAC study is the first to employ gold-standard measures of adiposity and insulin sensitivity, including dual energy x-ray absorptiometry, magnetic resonance imaging, and hyperinsulinemic-euglycemic glucose clamps, in antipsychotic-treated children. Preliminary results of the MEAC study, reported by Ginger E. Nicol, MD, at the recent APA meeting in San Francisco, CA (May 16–21), show significant changes in adiposity and insulin sensitivity during an initial course of antipsychotic treatment. Significant increases in percent body and total fat (p<0.0001) and decreases in insulin sensitivity (p<0.0001) were noted following treatment with all 3 antipsychotics, with clinically detectable changes in BMI percentile (p<0.001), fasting plasma triglycerides (p=0.001), and insulin (p=0.003). Drs. Newcomer and Nicol caution clinicians to carefully assess the risks and benefits of antipsychotic treatment in this patient population and suggest that clinically available markers, such as BMI percentile and fasting serum triglycerides, may be useful measures to monitor for adverse treatment-related metabolic changes in adiposity and insulin sensitivity, respectively.
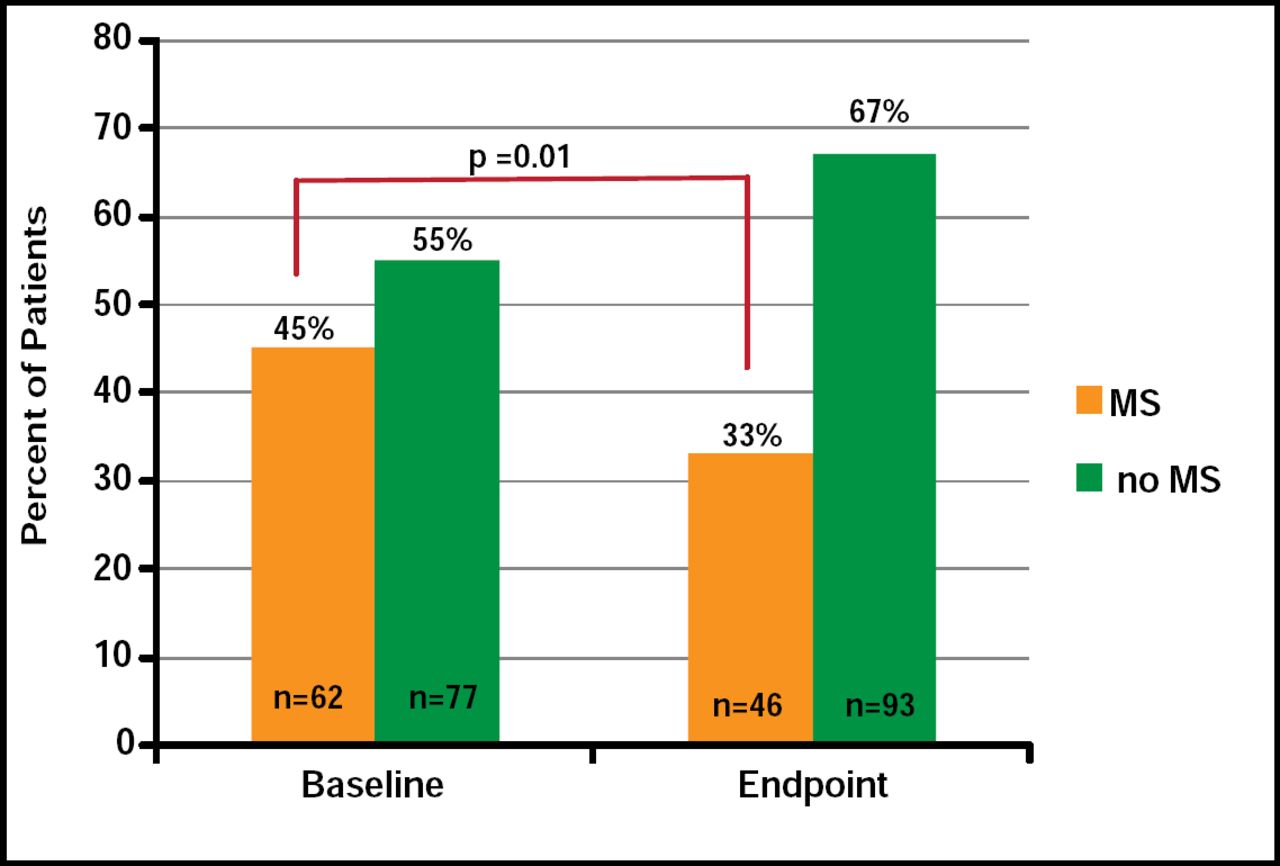
Previous studies have shown that the presence of obesity and other metabolic abnormalities affect the ability of treatment to stabilize patients who experience bipolar depressive episodes [Kemp DE et al. 2008 Meeting of Am Coll Neuropscyhopharmacology]. In contrast, data that were presented by David E Kemp, MD, Case Western Reserve University, Cleveland, OH, found no association between the presence of metabolic syndrome and reduced rates of acute stabilization following treatment with aripiprazole for 18 weeks. However, there was a significant decrease in the percentage of patients with the metabolic syndrome after aripiprazole treatment at the end of the stabilization phase compared with baseline (45% vs 33%; p=0.01; Figure 2).

Percentage of Patients with Metabolic Syndrome (MS) at Baseline and Endpoint Following 18 Weeks of Treatment with Aripiprazole.
The ability of aripiprazole to improve the profile of the metabolic syndrome was shown in another study that was presented by Sung-Wan Kim, MD, Chonnam National University Medical School, Gwangju, Republic of Korea. In this study, switching patients with schizophrenia from atypical antipsychotics to aripiprazole resulted in improved levels of total cholesterol (p<0.05), HDL (p<0.01), prolactin (p<0.001), and alanine aminotransferase (p<0.05) after 26 weeks of treatment (Figure 3).

Changes in Laboratory Parameters.
Despite recent improvements in treatments for schizophrenia, data from a variety of studies indicate that there are inconsistencies between the antipsychotics with respect to their effect on various components of metabolic risk. There remains a clear need for drug treatments with proven acute and maintenance efficacy and a neutral metabolic profile.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.