

Summary
Major depression is one of the most treatable medical illnesses. There is a strong correlation between anxiety symptoms and low rates of remission in patients with major depressive disorder (MDD) [Davidson JR, et al. Depress Anxiety 2002; Silverstone PH et al. Int Clin Psychopharmacol 2002]. This article discusses the role of anxiety in patients with major depressive disorder at the APA annual meeting.
- Anxiety Disorders
- Mood Disorders
Major depression is one of the most treatable medical illnesses. However, it is the fourth-most disabling medical condition worldwide, and it is predicted that by 2020 it will be second only to ischemic heart disease with regard to disability [National Institutes of Mental Health. How is Depression Detected and Treated? October 23, 2008; Rush AJ et al. Clinical Controlled Trials 2004]. There is a strong correlation between anxiety symptoms and low rates of remission in patients with major depressive disorder (MDD) [Davidson JR, et al. Depress Anxiety 2002; Silverstone PH et al. Int Clin Psychopharmacol 2002]. John Zajecka, MD, Rush University Medical Center, Chicago, IL, discussed the role of anxiety in patients with major depressive disorder at the APA annual meeting.
Anxious depression is associated with greater functional impairment, increased risk of suicide, and higher rates of treatment interruption or discontinuation [Jaffe RT et al. Am J Psychiatry 1993; Clayton P et al. Am J Psychiatry 1991; Flint AJ et al. Am J Geriatr Psychiatry 1997]. There are a variety of anxiety symptoms that may present in MDD patients, such as phobic symptoms, panic attacks, obsessive-compulsive tendencies, somatic anxiety, and worry, although differentiating between comorbidity versus secondary anxiety remains an issue. In a study by Fava and colleagues, comorbid anxiety diagnoses were present in 50.6% of MDD patients (27% social phobia, 16.9% simple phobia, 14.5% panic disorder, 10.6% generalized anxiety disorder, 6.3% obsessive-compulsive disorder, and 5.5% agoraphobia) [Fava M et al. Compr Psychiatry 2000]. A similar study by Zimmerman and colleagues demonstrated that 56.8% of patients with MDD (n=307) had comorbid anxiety disorders [Zimmerman M et al. J Clin Psychiatry 2002].
Prof. Zajecka noted that anxious depression is associated with greater morbidity and mortality rates compared with depression without anxiety. Therefore, it is important to treat both the anxiety and the depression in order to reach remission. “It can be difficult, but it should be possible for most, if not all, [MDD patients with anxious depression] to achieve remission,” said Prof. Zajecka.
Depression and anxiety disorders have been linked to abnormalities in norepinephrine (NE) signaling, serotonin (5HT) activity, corticotrophin-releasing hormone (CRH), and glucocorticoid stress response abnormalities [Ressler KJ et al. Depress Anxiety 2000]. Audrey Tyrka, MD, PhD, Brown Medical School and Butler Hospital, Providence, RI, discussed these neurobiological pathways and how they relate to anxious depression.
5-HT activity may influence the amygdala region of the brain, which is associated with intense and fearful emotion, including pathological anxiety. In a study by Caspi and colleagues that investigated gene-environmental interaction, individuals who had 1 or 2 copies of the short allele of the 5-HT promoter polymorphism exhibited more depressive symptoms, diagnosable depression, and suicidality in relation to stressful life events than individuals who were homozygous for the long allele [Caspi A et al. Science 2003]. Additionally, a pooled analysis by Hariri and colleagues found that 5-HT affects the development of a broader corticolimbic circuit and alters the functional integration of emotional information between the amygdala and medial prefrontal cortex [Hariri AR et al. Biol Psychiatry 2006]. These results suggest that 5-HT may be a predictive biomarker of increased risk for mood disorders, such as anxious depression.
The hypothalamic-pituitary-adrenal (HPA) axis activates the body's fight-or-flight reaction. HPA axis abnormalities, such as extreme fluctuation in glucocorticoid receptor density or negative feedback inhibition, fluctuation in basal cortisol concentrations, and increased CRH within the cerebral spinal fluid, have been implicated in anxiety and depression [Duman RS et al. Arch Gen Psychiatry 1997; Heim C et al. Arch Gen Psychiatry 2009; Risbrough VB & Stein MB. Horm Behav 2006; Smoller JW et al. Biol Psychiatry 2005]. Additionally, the HPA axis and the CRH gene may also be linked to behavioral inhibition, such as the tendency to withdraw or avoid new situations, often found in patients with anxious depression [Smoller JW et al. Biol Psychiatry 2005; Tyrka AR et al. Acta Psychiatr Scand 2007; Tyrka AR et al. Horm Behav 2008].
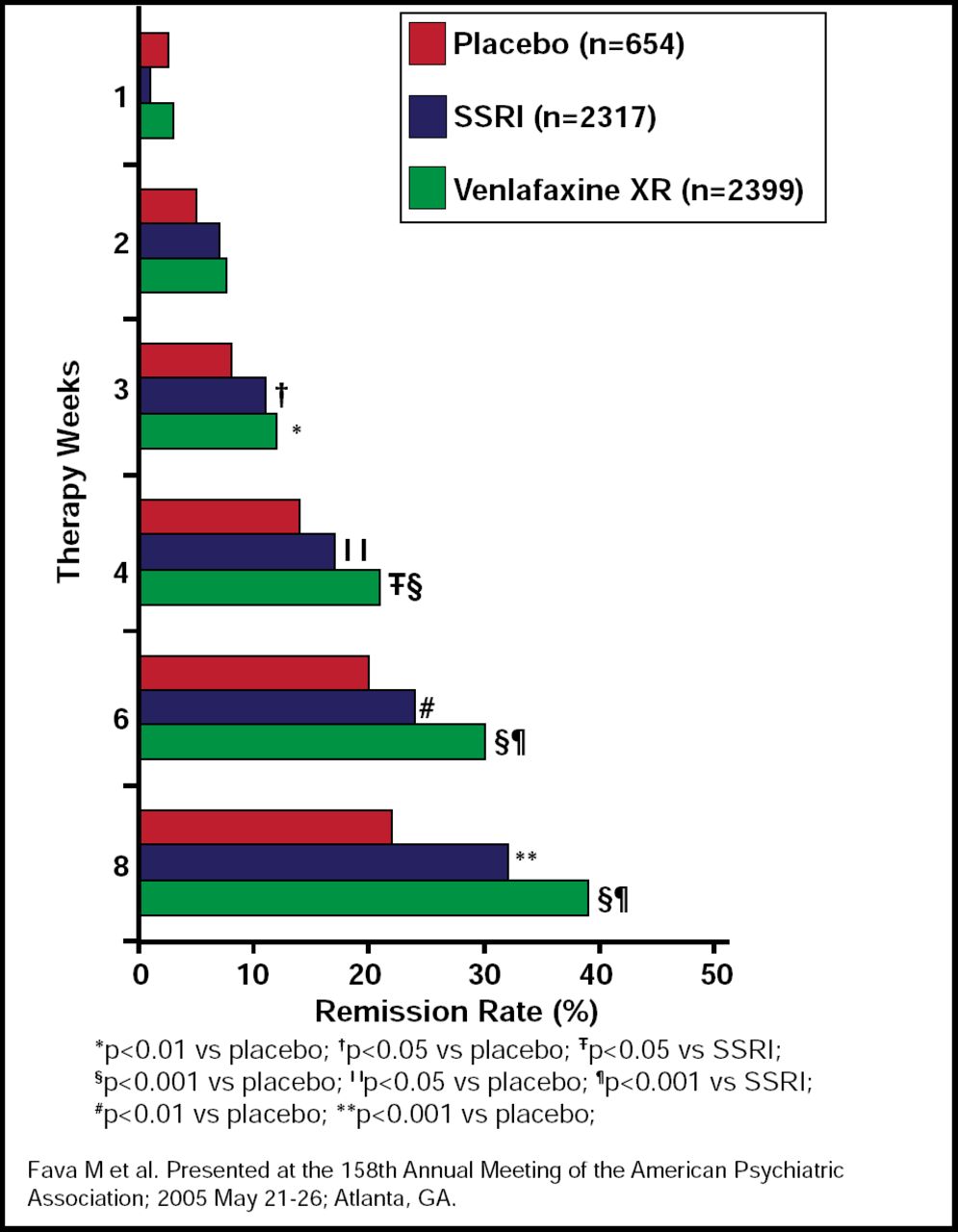
Maurizio Fava, MD, Massachusetts General Hospital, Boston, MA, discussed pharmacotherapeutic strategies for the treatment of anxious depression. There are various pharmacological approaches for anxious depression, including monotherapy with antidepressants and augmentation with agents, such as benzodiazepines, eszopiclone, buspirone, anticonvulsants, and antipsychotics. Published studies have shown that there is no significant difference between the use of tricyclics and SSRIs for anxious depression [Tollefson GD et al. J Clin Psychopharmacol 1994; Marchesi C et al. Pharmacopsychiatry 1998; Versiani M et al. Int Clin Psychopharmacol 1999; Sheehan D et al. Psychopharmacol Bull 1992; Russell JM et al. Depress Anxiety 2001; Moon CAL et al. J Psychopharmacol 1994]. To date, there is no FDA-approved indication for the use of antidepressants for the treatment of anxious depression. However, in a pooled analysis of 31 studies by Fava and colleagues, remission rates at 8 weeks in patients who were treated with venlafaxine (an SNRI) for anxious depression were significantly better than SSRI or placebo (p<0.001 for venlafaxine vs SSRI and placebo; Figure 1) [Fava M et al. 158th Annual Meeting of the American Psychiatric Association 2005].

Pooled Analysis of Remission Rates Across 31 Studies of Venlafaxine Versus SSRIs Versus Placebo in Anxious Depression.
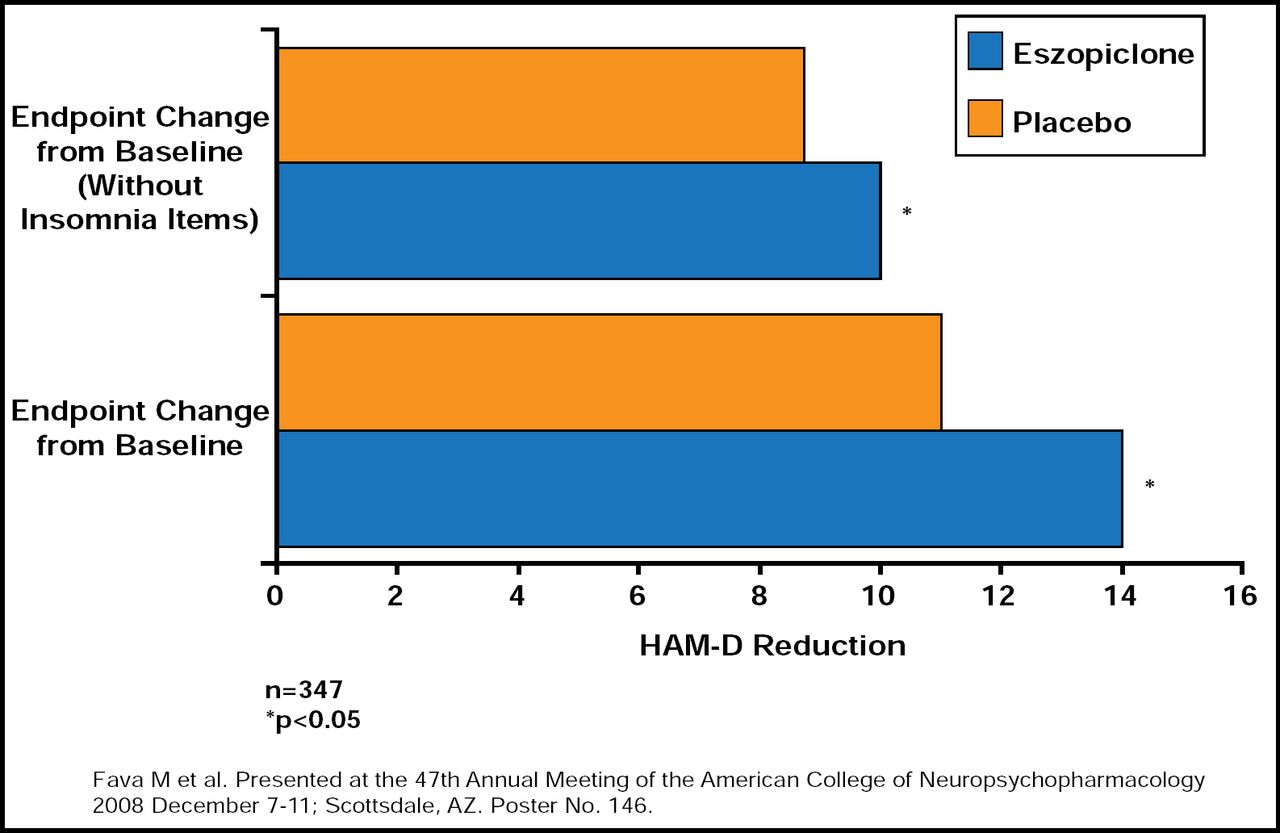
Another pooled analysis by Fava and colleagues that compared eszopiclone augmentation versus placebo demonstrated improvement in HAM-D scores for patients with anxious depression (p<0.05; Figure 2) [Fava M et al. 47th Annual Meeting of the American College of Neuropsychopharmacology 2008].

Pooled Analysis of Trials Comparing Eszopiclone Added to SSRI and Placebo in Anxious Depression.
Although antidepressants are typically equally effective in anxious depression, this population tends to do poorly across the board. Patients with anxious depression do significantly worse than nonanxious MDD patients, regardless of treatment strategy [Fava M et al. Am J Psychiatry 2008]. Anxiolytics may be indicated in nonresponders. However, side effect management is important. “Monotherapies have modest effect; therefore, there is a need for novel therapies targeting this population,” said Prof. Fava.
Another strategy for the treatment of anxious depression is cognitive behavioral therapy (CBT). Amy Farabaugh, PhD, Massachusetts General Hospital, Boston, MA, pointed out that cognition, behavior, and biochemistry are all important components of MDD and anxiety. In a study by Brown and colleagues, MDD patients with comorbid anxiety disorders tended to terminate treatment more frequently than those with depression alone [Brown C et al. Am J Psychiatry 1996]. This creates treatment barriers for the clinician. However, a preliminary analysis of STAR*D that evaluated CBT for anxious depression suggests that CBT is equally efficacious in patients with anxious and nonanxious depression; the rate of treatment continuation was similar for both groups [Farabaugh A et al. Manuscript in preparation].
According to Prof. Farabaugh, an important part of CBT in the patient with anxious depression is to start with small goals so that the patient is encouraged and notices progress early in the treatment. Recognizing symptoms that may lead to early treatment termination is also essential. A thorough clinical interview and careful classification of symptoms are therefore necessary. The patient's perception of how he is affected by each symptom plays a large role in CBT and should be considered and discussed.
Conceptualization throughout the course of therapy, such as helping the patient understand the relationship between the anxiety and depressive symptoms, is a valuable strategy in CBT. Because depression and anxiety may occur concurrently, it is helpful to consider skills and therapy that will complement both aspects of MDD. Prof. Farabaugh concluded that the integration of psychosocial and pharmacological approaches in these patients should be considered in order to establish remission. “We still have a lot to learn in terms of optimizing treatment strategies, but it does look like combining psychotherapy with pharmacotherapy may be helpful in patients with anxious depression,” said Prof. Farabaugh.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.