

Summary
Although first described in battle reports as early as the 6th century, posttraumatic stress disorder (PTSD) only entered the DSM lexicon in 1980. Despite being most often associated with veterans and the military, PTSD is not uncommon after many types of traumatic events, such as car accidents, natural disasters, and violent deaths. This article discusses the impact of PTSD on soldiers and their families and treatments that are currently available.
- Psychiatry Clinical Trials
- Anxiety Disorders
Although first described in battle reports as early as the 6th century, posttraumatic stress disorder (PTSD) only entered the DSM lexicon in 1980. In DSM-IV, it is described as an anxiety disorder that follows exposure to extreme psychological trauma that involves someone's death, a threat of death or harm, serious physical injury, an unwanted sexual act, or a threat to physical or psychological integrity. Despite being most often associated with veterans and the military, PTSD is not uncommon after many types of traumatic events, such as car accidents, natural disasters, and violent deaths. The DSM-IV defines the event as involving intense fear, helplessness, or horror (in children, the response must involve disorganized or agitated behavior). Diagnostic symptoms include a reexperience of the event through flashbacks and nightmares; avoidance of stimuli that are associated with the trauma; increased arousal, such as difficulty falling or staying asleep; anger and hypervigilance; and numbing of general responsiveness that last more than 6 months and cause significant impairment in social, occupational, or other important areas of functioning.
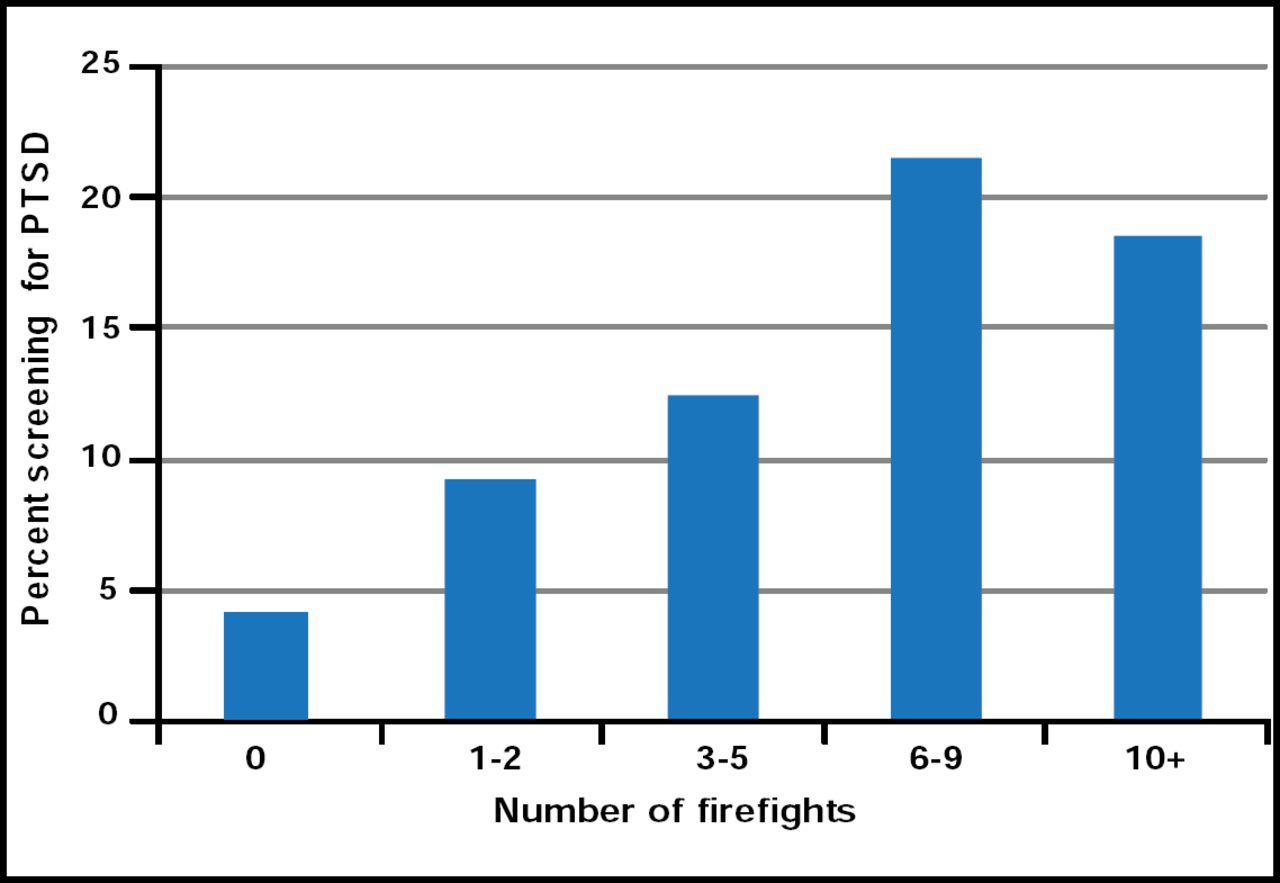
In a Presidential Symposium, Robert J. Ursano, MD, Uniformed Services University of the Health Sciences, Bethesda, MD, discussed the impact of PTSD on soldiers and their families and treatments that are currently available. He noted that for soldiers who were involved in combat operations in Iraq and Afghanistan, length of exposure to trauma was the chief determinant of whether or not they developed PTSD. The more firefights that an individual experiences, the greater the risk for PTSD (Figure 1).

Percent Screening Positive for PTSD By Number of Firefights.
Five percent of the soldiers who returned from Afghanistan and 12.9% who returned from Iraq screened positive for PTSD. However, less than 40% sought treatment, often citing possible stigma that might affect their careers. Failure to make prompt initial treatment contact is pervasive in the mental health field. Lifetime probability of treatment contact for PTSD is 65%, wherein only 7% make contact within 1 year of PTSD onset. The median delay to first treatment contact is 12 years [Wang PS et al. Arch Gen Psychiatry 2005].
PTSD rarely occurs in isolation. Long-term follow-up studies have shown associations between combat-related PTSD and alcohol abuse, depression, antisocial personality disorder, and early-age cardiac mortality. In a 30-year follow-up study of ∼8000 Vietnam combat veterans, individuals who were initially diagnosed with PTSD, but who were free of heart disease at baseline, had a 20% increased risk of heart disease-related mortality, even after controlling for traditional risk factors [Boscarino J. Ann Epidemiol 2005].
Treatment is multifaceted and occurs across many domains: the disorder itself, symptoms, impairment of function, disability, comorbid conditions, and trajectory of the condition. Cognitive behavioral therapy, eye movement desensitization and reprocessing (EMDR), and selective serotonin reuptake inhibitors (SSRIs) have been shown to speed recovery and prevent PTSD in rape and accident victims, whereas combat-related PTSD is most effectively treated with cognitive behavioral therapy. Current evidence indicates that single-session, individual psychological debriefing immediately after a trauma may worsen the symptoms of the individual and is not recommended.
Several lines of research suggest that in PTSD the noradrenergic system is dysregulated. PTSD patients have significantly higher baseline norepinephrine levels and a blunted norepinephrine response to postural challenge compared with normal subjects. Noradrenergic dysregulation could lead to one to reexperience symptoms. In addition, exaggerated activity of the amygdala in conjunction with reduced activation in the medial prefrontal cortex and increasing dysfunction of the hippocampusis consistently reported in PTSD patients. These changes are thought to interfere with extinction of the fear response, arousal, memory, and normal sleep cycles. Dr. Ursano believes that we are on the forefront of a new understanding of these neurobiological mechanisms—an understanding that will lead to better treatments.
PTSD, combined with alcohol abuse, is associated with lower functioning and worse treatment outcome than either disorder alone. This comorbid condition is receiving special attention, because PTSD and alcohol abuse are common in many veterans who return from Iraq and Afghanistan. Thomas R. Kosten, MD, Baylor College of Medicine, Houston, TX, described PTSD as a disruption in the delicate balance between the capacity to think critically and maintenance of a level of arousal that does not overpower that capacity. Hormonally, this balance is maintained by norepinephrine (the revving-up hormone) and cortisol (the quieting-down hormone). Both are released in response to stress, but they get out of balance in PTSD.
Many of these neural circuits overlap with the memory circuits that are involved in addiction, which Dr. Kosten referred to as a disease of memory. Both fear (PTSD) and drug-seeking are learned or conditioned responses that can lead to maladaptive behavior when expressed inappropriately, manifesting as anxiety disorders and addiction, respectively. Extinction therapy, a form of inhibitory learning that suppresses a previously conditioned response, is hailed as a promising new treatment approach. The memory pathways that are associated with glutamate may facilitate the extinction process, whereby the PTSD/alcoholic subject creates a new nonreinforcing association of behavior instead of retrieving the old associations.
Despite a broad range of PTSD target symptoms (eg, experiencing avoidance, numbing, and hyperarousal), a 2008 Institute of Medicine Report concluded that evidence is inadequate to determine efficacy for any class of agents that are currently used in treatment. However, that does not mean that treatment is not efficacious, according to Kathleen Brady, MD, Medical University of South Carolina, Charleston, SC.
Two double-blind placebo-controlled studies confirmed the efficacy of sertraline, an SSRI, for severe chronic PTSD in civilians. Patients who received sertraline experienced a 5% relapse rate compared with 26% for placebo patients. The ability of sertraline to sustain improvement was comparable across the 3 core PTSD symptom clusters (reexperiencing/intrusion, avoidance/numbing, and hyperarousal) [Davidson J et al. Am J Psychiatry 2001]. In another study, sertraline was significantly (p<0.05) more effective than placebo after 12 weeks of treatment for the PTSD symptom clusters of avoidance/numbing and increased arousal but not for reexperiencing/intrusion [Brady K et al. JAMA 2000]. However, sertraline has not been shown to be effective for veterans with combat-related PTSD, maybe because of a higher baseline PTSD severity in this group of patients [Zohar J et al. J Clin Psychopharmacology 2002; Friedman MJ et al. J Clin Psychiatry 2007].
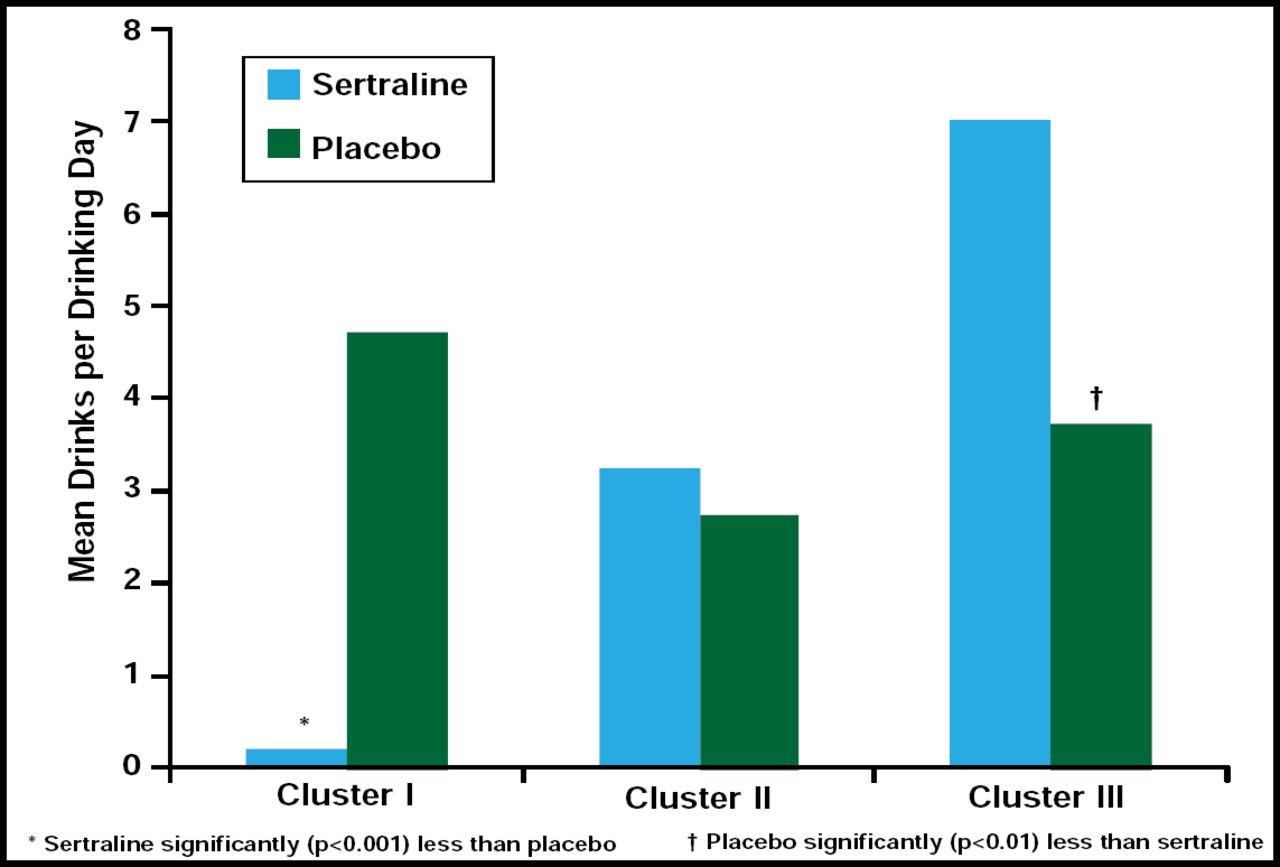
One study showed that sertraline might be an effective treatment for a certain cluster of patients who have PTSD that cooccurs with alcohol abuse. Although there was a significant decrease in alcohol use during the trial in both the sertraline and the placebo groups, sertraline-treated participants with less severe alcohol dependence and early-onset PTSD (Cluster I) had significantly fewer drinks per day (p <0.001) compared with placebo-treated patients. For participants with more severe alcohol dependence and later-onset PTSD (Cluster III), the placebo group had significantly fewer drinks per day (p <0.01; Figure 2) [Brady K et al. Alcohol Clin Exp Res 2005].

Effect of Sertraline in PTSD Patients with Co-occurring Alcohol Abuse.
In the closing panel discussion, it was mentioned that more refractory patients were showing up for treatment, many with comorbid conditions. Getting returning combat soldiers into therapy or getting those who do enter therapy engaged in the process were mentioned as major problems. The internet and virtual reality were discussed as possible engaging tools, because they offer a certain amount of anonymity.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.