

Summary
Alcohol use disorders present a widespread and serious public health problem in the United States. The disparity between the prevalence of this disorder and the number of persons who receive treatment indicates a huge gap in terms of evidence-based care. Likewise, individuals with psychiatric illness, particularly those with severe disorders, have rates of smoking addiction that are 2 to 3 times higher than the general population. This article discusses advances in alcohol and tobacco dependence.
- Psychiatry Clinical Trials
- Smoking Cessation
- Substance-Related Disorders
Advances in Alcohol and Tobacco Dependence
Alcohol use disorders present a widespread and serious public health problem in the United States (US). Results of an epidemiological study that used DSM-IV criteria to examine the lifetime and 12-month prevalence of alcohol use disorders in the United States during 2001–2002 showed that 8.5% of adults had experienced alcohol use disorders in the prior 12 months (4.7% abuse, 3.8% dependence) and that 30.3% experienced alcohol use disorders during their lifetimes (17.8% abuse, 12.5% dependence). Only 24.1% of those with alcohol dependence were ever treated [Hasin DS et al. Arch Gen Psychiatry 2007]. The disparity between the prevalence of this disorder and the number of persons who receive treatment indicates a huge gap in terms of evidence-based care.
Hugh Myrick, MD, discussed the approach to treatment that is used at the Medical University of South Carolina, Charleston, SC, as well as several recent studies on the use of anticonvulsants in the treatment of alcoholism.
The majority of alcohol withdrawal treatment is now done on an outpatient basis, using decreasing doses of benzodiazepines over 4 to 7 days. As a class, the benzodiazepines are subject to abuse, however, and in addition, recent studies have shown that they may prime alcoholics to drink [Poulos & Zack. Behav Pharm 2004]. Researchers have been studying anticonvulsants as an alternative to benzodiazepines for alcohol detoxification since the 1970s. Dr. Myrick presented data from 2 studies in which an anticonvulsant was compared with a benzodiazepine.
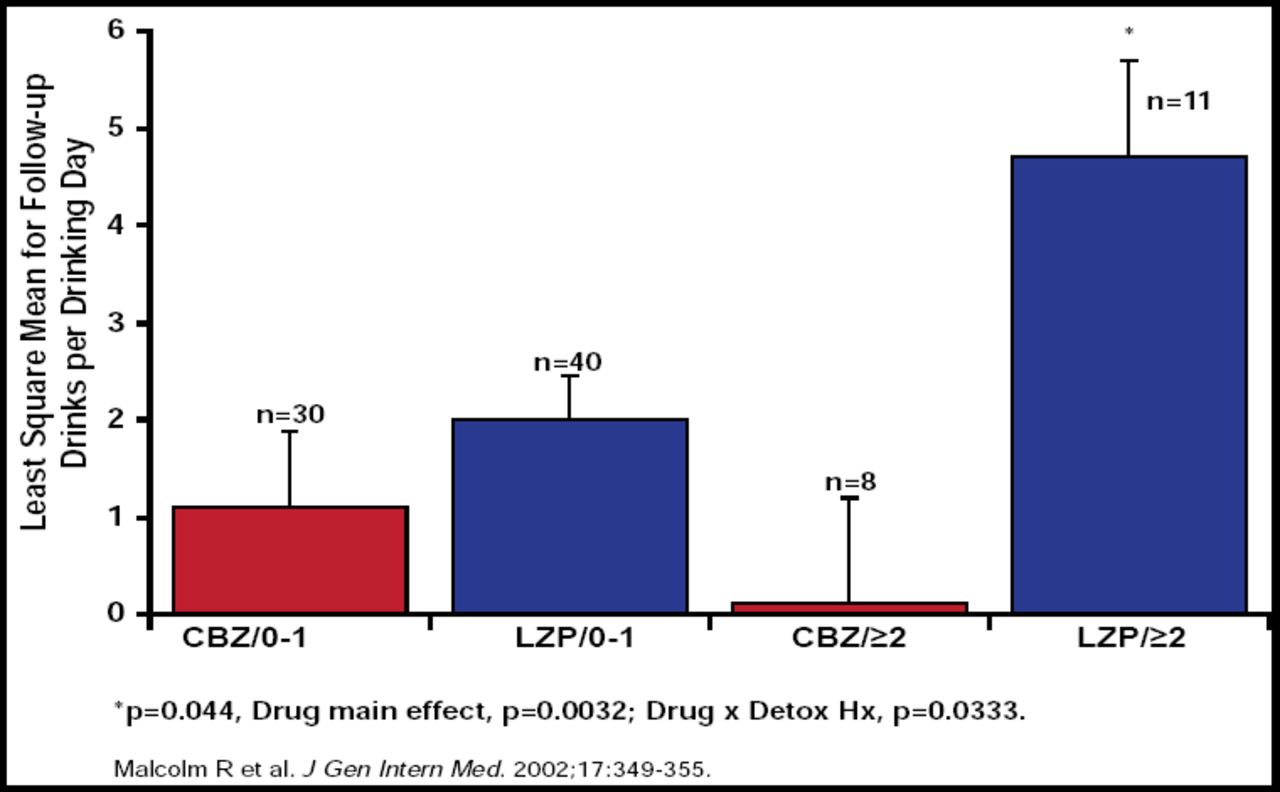
Results from a double-blind, outpatient trial (n=136) that compared 5-day tapering doses of carbamazepine (600 to 800 mg/day tapered to 200 mg/day) with lorazepam (6 to 8 mg/day tapered to 2 mg/day) showed that both drugs were effective in decreasing the symptoms of alcohol withdrawal. However, carbamazepine was superior to lorazepam in preventing rebound withdrawal symptoms and reducing post treatment drinking, particularly for those with a history of ≥2 prior medicated detoxifications (Figure 1) [Malcolm R et al. J Gen Int Med 2002]. Results from another study that compared gabapentin with lorazepam showed similar efficacy between the 2 medications in reducing alcohol symptoms but significantly (p≥0.05) lower odds of drinking in the low-dose gabapentin group versus lorazepam [Myrick H et al. Alcohol Clin Exp Res 2009].

Drinks per Drinking Day: Day 6 to Day 12.
Four treatments are currently approved by the FDA to treat alcohol dependence: disulfiram (Antabuse®), naltrexone (ReVIa®), acamprosate (Campral®), and extended-release injectable naltrexone (Vivitrol®). As with many chronic diseases, adherence is an issue with alcoholism. Medication discontinuations are high, and 1 study of naltrexone has shown that ∼50% of patients do not refill their prescription even once [Harris KM et al. Psychiatr Serv 2004]. Nonadherent patients are more likely to have significantly more inpatient detoxification admissions, nonalcohol-specific hospital admissions, and nonalcohol-specific ER visits and no counseling participation [Stephenson et al. Am Acad Addiction Psychiatry 2006 Annual Meeting]. Once-monthly injections of extended-release naltrexone have been shown to prolong initial abstinence and reduce heavy drinking days in alcohol-dependent adults [Garbutt JC et al. JAMA 2005; O'Malley SS et al. J Clin Psychopharmacol 2007] and may increase adherence with medication [Un H. Addiction Health Services Research 2008 Annual Meeting].
Individuals with psychiatric illness, particularly those with severe disorders, have rates of smoking addiction that are 2 to 3 times higher than the general population [Morisano D et al. Can J Psychiatry 2009]. They also have more difficulty quitting (success rates of ∼one-third of the general population). Recent data show that tobacco smoking accounts for as much as 50% of the reduction in life expectancy that is seen in persons with psychiatric disorders, such as schizophrenia and bipolar disorder [Hennekens CH et al. Am Heart J 2005]. Tony P. George, MD, FRCPC, University of Toronto and The Centre for Addiction and Mental Health, Toronto, Ontario, Canada, discussed some of the approaches that can be used to assist these individuals with smoking cessation.
A number of barriers to effective treatment of nicotine dependence exist, some of which are particularly relevant to persons with psychiatric disorders, including the limited access to smoking cessation services for the mentally ill and the rarity of smoke-free living environments for these individuals. Further, a substantial proportion of the staff at mental health centers are current smokers themselves, and it has been shown that current smokers are less likely than those who have quit to refer patients for smoking cessation treatment [Weinberger et al. J Addict Dis 2008].
Although all smokers should be offered cessation therapy, the best candidates for pharmacotherapy are daily smokers (at least >10 cigarettes/day) who show evidence for moderate to heavy levels of nicotine dependence (eg, Fagerstrom Test of Nicotine Dependence [FTND] score >5), are willing to comply with daily medication dosing, and accept basic cessation counseling during the medication trial. There are 3 classes of pharmacotherapy for tobacco dependence: nicotine replacement therapies (NRTs), the antidepressant bupropion (in the sustained release formulation), and the nicotinic partial agonist varenicline (Figure 2). Several new tobacco pharmacotherapies, such as corticotropin releasing factor (CRF) antagonists, glutamate modulating agents, monoamine oxidase inhibitors, γ-aminobutyric acid (GABA-B) receptor agonists, and nicotine vaccines, are on the horizon.

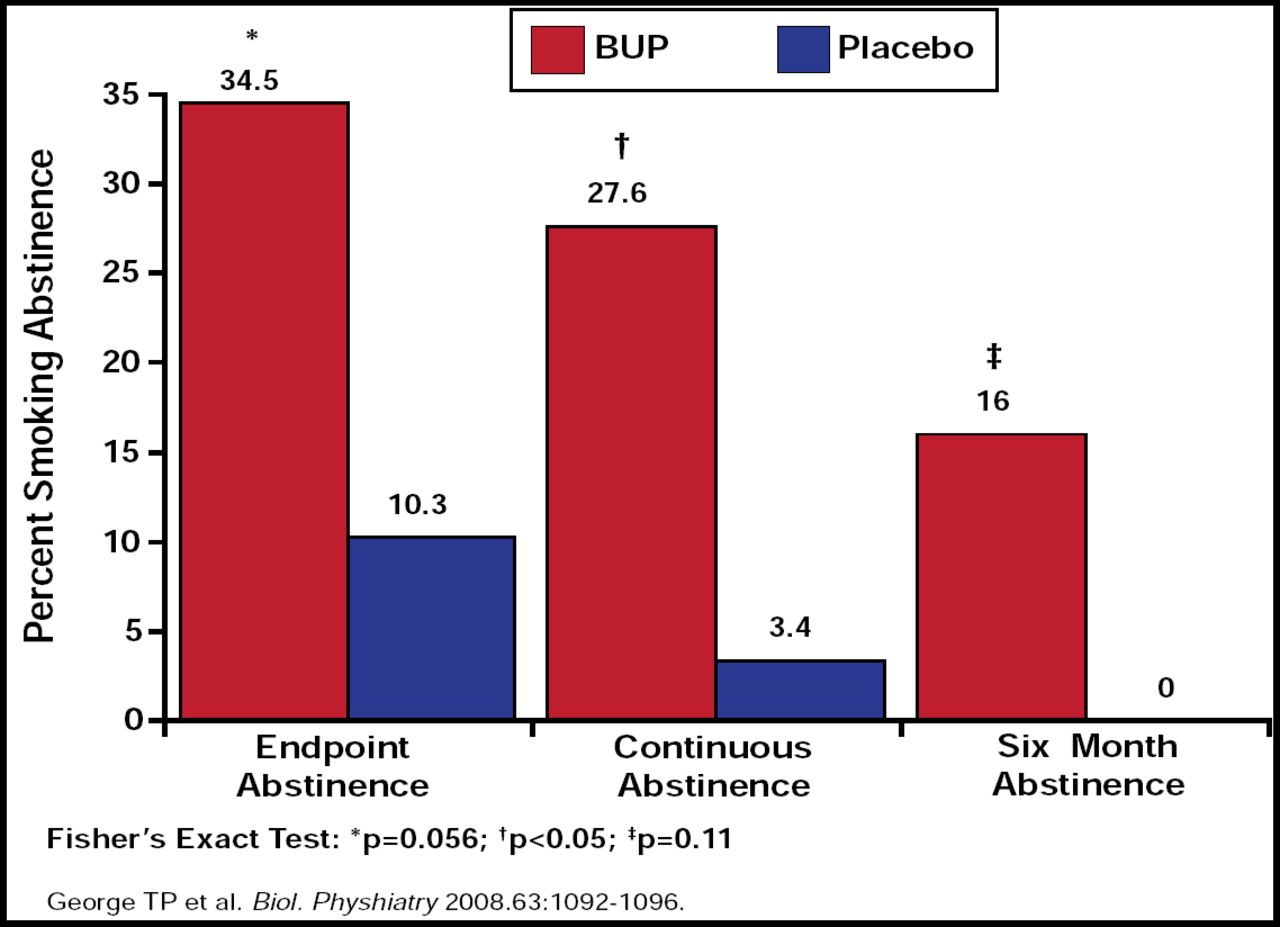
Smoking Abstinence.
As with many medical conditions, combination therapy for smoking cessation is now being evaluated in clinical studies. Dr. George presented the results of a 10-week, double-blind, placebo-controlled trial in which outpatients with schizophrenia who were also smokers were treated with either sustained-release bupropion 300 mg/day plus a nicotine patch (21 mg/24 h; n=29) or the patch alone (n=29). The primary endpoints were continuous smoking abstinence in the last 4 weeks of the trial and 7-day point prevalence abstinence 6 months after the target quit date. The results at the 7-day point prevalence endpoint were similar for both treatments; however, smokers who received the combination treatment were significantly (p<0.05) more likely to achieve continuous smoking abstinence (8/29, 27.6%) than those who were treated with the patch alone (1/29, 3.4%). Neither bupropion SR nor smoking abstinence significantly altered the positive or negative symptoms of schizophrenia. The combination was well tolerated in smokers with schizophrenia [George TP et al. Biol Psychiatry 2008]. Several other studies on treating tobacco addiction in other psychiatric disorders (eg, major depression, posttraumatic stress disorder, and bipolar 1 disorder) are ongoing and hopefully will provide guidance on how to approach smoking cessation in this difficult-to-treat population.
In summary, Dr. George said psychiatrists need to identify cigarette smokers in their practice, assess motivation to quit, and either treat these patients or refer them for treatment.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.