

Summary
Recently, options for the endovascular treatment of peripheral vascular disease—including carotid artery disease, renal artery disease, and peripheral artery disease of the legs—have expanded dramatically. In general, physicians tend to use endovascular techniques for first-line therapy and reserve surgery for more complex cases. This article discusses the benefits and drawbacks of optimal medical therapy compared with endovascular or surgical approaches to vascular disease.
- Interventional Techniques & Devices
- Hypertensive Disease
- Renal Artery Obstruction
- Renal Disease
Recently, options for the endovascular treatment of peripheral vascular disease—including carotid artery disease, renal artery disease, and peripheral artery disease of the legs— have expanded dramatically. In general, physicians tend to use endovascular techniques for first-line therapy and reserve surgery for more complex cases. In this presentation, Michael R. Jaff, DO, Massachusetts General Hospital, Boston, MA, discussed the benefits and drawbacks of optimal medical therapy compared with endovascular or surgical approaches to vascular disease.
Carotid Artery Disease
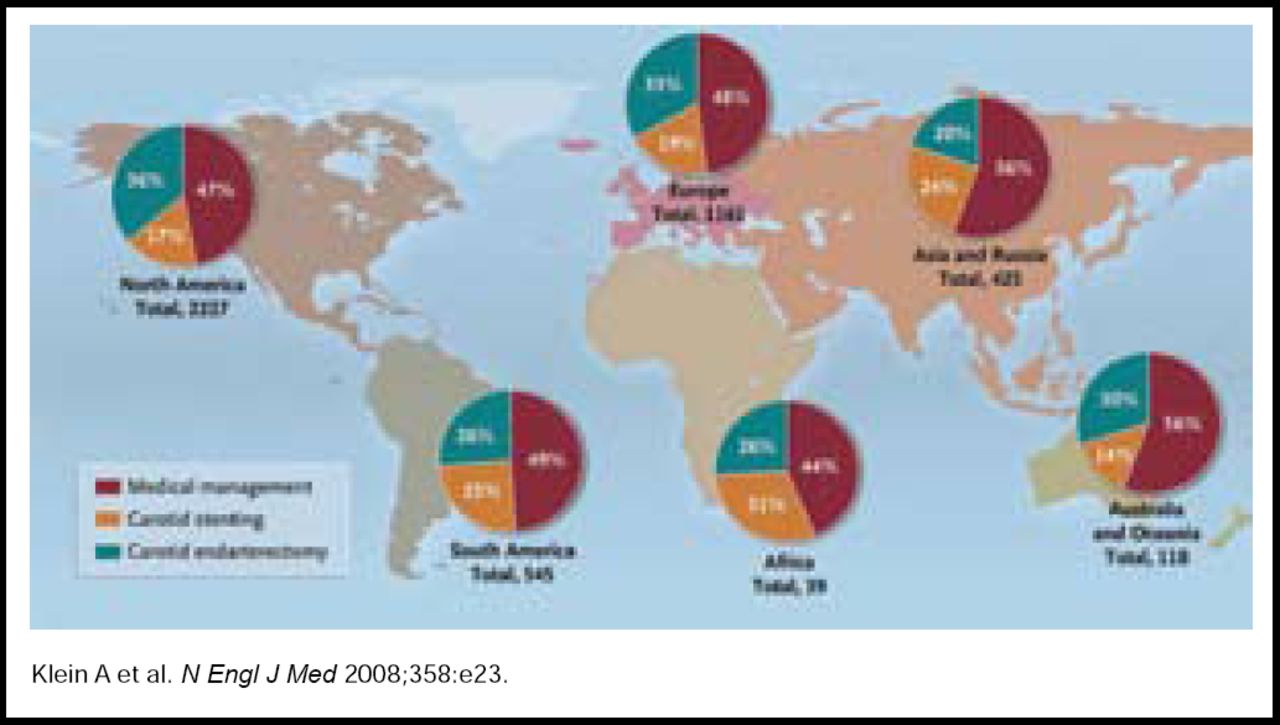
Currently, there is no consensus regarding the optimal treatment for carotid stenosis. In a 2008 poll of New England Journal of Medicine readers worldwide, approximately 49% said that they favored aggressive medical management as first-line treatment. Remaining respondents favored either carotid endarterectomy (31%) or stenting (20%) (Figure 1). When surgery or stenting is chosen, survey respondents commented that the selection of an experienced surgeon or interventionalist who has a history of low complication rates is critical to achieving the best possible outcome [Klein A et al. N Engl J Med 2008].

Worldwide Preferences for the Management of Carotid Artery Disease.
Copyright © Massachusetts Medical Society 2008. All rights reserved.
Ongoing trials may help to determine the optimal treatment approach in select patient subgroups, Dr. Jaff said. The Carotid Revascularization Endarterectomy versus Stenting Trial (CREST), which is expected to report preliminary results by early 2010, may help clarify the best approach for standard-risk symptomatic or asymptomatic patients. The Asymptomatic Carotid Trial (ACT 1) and Asymptomatic Carotid Surgery Trial 2 (ACST 2) will also compare carotid artery stenting with carotid endarterectomy in standard-risk, asymptomatic patients.
Renal artery disease
To date, the optimal intervention for patients with atherosclerotic renal artery stenosis has not been determined. In 2006, a systematic review of clinical trial data, commissioned by the Agency for Healthcare Research and Quality (AHRQ), concluded that the available evidence does not clearly support renal artery revascularization over medical treatment for the treatment of renal artery stenosis [Balk E et al. Ann Intern Med 2006].
Based on current data, renal intervention should be offered as a treatment option only after a reasonable trial of optimal antihypertensive therapy fails to normalize blood pressure. In addition, patient history must demonstrate that blood pressure cannot be controlled with pharmacological therapy alone and that chronic kidney disease is due to renal ischemia rather than another cause. Ideally, treatment of renal artery disease should help normalize blood pressure, maintain renal function, and reduce the long-term risk of cardiovascular events and mortality.
Renal artery revascularization is not likely to gain widespread support without rigorous head-to-head comparison with optimal medical treatment, Dr. Jaff said. The Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) trial is designed to determine whether best medical therapy that is combined with stenting of hemodynamically significant renal artery stenosis in patients with systolic hypertension can reduce the incidence of adverse cardiovascular and renal events compared with best medical therapy alone. Findings from CORAL may determine the future of revascularization for patients with renal artery stenosis.
Peripheral Artery Disease
Peripheral artery disease (PAD) is associated with an increase in the risk of coronary artery and cerebrovascular disease, suggesting that the effective management of PAD has broad implications for overall cardiovascular health. Peripheral endovascular revascularization has been shown in certain series to lead to significant and sustained improvements in symptoms, physical function, and quality of life in patients with symptomatic disease [Safley DM et al. Circulation 2007].
Technological advances have expanded revascularizaton options for patients with PAD. Stent implantation for disease of the superficial femoral artery has been associated with high rates of late clinical failure. Therefore, percutaneous transluminal angioplasty has been the preferred technique for endovascular treatment, particularly in short (<7 cm) lesions, with stent deployment recommended only in the event of suboptimal technical results. However, recent data have shown that primary implantation of a self-expanding nitinol stent is more effective than primary balloon angioplasty in preventing restenosis at 6 months and improving treadmill testing outcomes at 6 and 12 months [Schillinger M et al. N Engl J Med 2006].
Recent data also suggest that drug-coated balloons provide a promising option for the treatment of PAD. In a pilot trial of 87 patients with PAD, paclitaxel-coated balloon catheters reduced restenosis compared with standard balloons and caused no obvious adverse events in patients who were undergoing angioplasty of the femoropopliteal arteries [Werk M et al. Circulation 2008].
In conclusion, Dr. Jaff cautioned that technically successful procedures do not always translate into clinically important improvements. Future trials should incorporate clinically meaningful endpoints, such as walking distance, ulcer healing, and prevention of limb loss, to demonstrate the true clinical benefits of revascularization.
State-of-the-Art Revascularization Therapy: Multivessel and Left Main Disease
Coronary artery bypass grafting (CABG) remains the standard of care for patients with left main or multivessel coronary artery disease. However, for a subset of patients, percutaneous coronary intervention (PCI) is as safe and effective as CABG. In this presentation, Marie-Claude Morice, MD, Institut Hospitalier, Massy, France, compared CABG and PCI for patients with left main or multivessel coronary artery disease.
Improvements in PCI, especially the advent of drug-eluting stents (DES), have led to an increase in the use of PCI in patients who are candidates for either PCI or CABG. The most recent trial to compare these procedures, the Synergy between PCI with Taxus and Cardiac Surgery (SYNTAX) study, provides important lessons regarding revascularization in the patient population, Professor Morice said.
In the international SYNTAX trial, 1800 patients with 3-vessel or left main coronary artery disease were randomly assigned to either revascularization with CABG (n=897) or PCI (n=903) that involved DES. Patients enrolled in the SYNTAX trial had complex disease, including bifurcation in 72% of patients, medically treated diabetes in approximately 25% of patients, and more than 4 lesions on average. The primary endpoint was any major adverse cardiac or cerebrovascular event (MACCE), including death from any cause, stroke, MI, or repeat revascularization.
After 1 year, the risk of MACCE was significantly higher in the PCI group than in the CABG group (17.8% vs 12.4%; p=0.002), due primarily to an increase in the rate of repeat revascularization (13.5% vs 5.9%; p<0.001). Conversely, the risk of stroke was significantly higher in the CABG group than in the PCI group (2.2% vs 0.6%; p=0.003). However, the noninferiority criteria were not met for the SYNTAX trial, because the primary endpoint of MAACE was significantly higher for PCI [Serruys PW et al. N Engl J Med 2009].
Findings from SYNTAX suggest that CABG should remain the standard of care for patients with left main or multivessel coronary artery disease. However, PCI is an excellent alternative to CABG in some patients, Professor Morice said. Future trials will seek to identify which patients are most likely to benefit from PCI.
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.