

Summary
There has been a significant increase in the consumption of refined sugars across the globe over the past 20 years, with the main source of this increase from sugar-sweetened beverages, including soft drinks, fruit drinks, energy drinks, and vitamin and other functional beverage waters. This article presents new updates on the relationship between sugar-sweetened beverages and the metabolic syndrome.
- Cardiometabolic Disorder
- Nursing
At the recent 3rd International Congress on Prediabetes and the Metabolic Syndrome in Nice, France, opinion leaders gathered during a dedicated symposium to present new updates on the relationship between sugar-sweetened beverages and the metabolic syndrome.
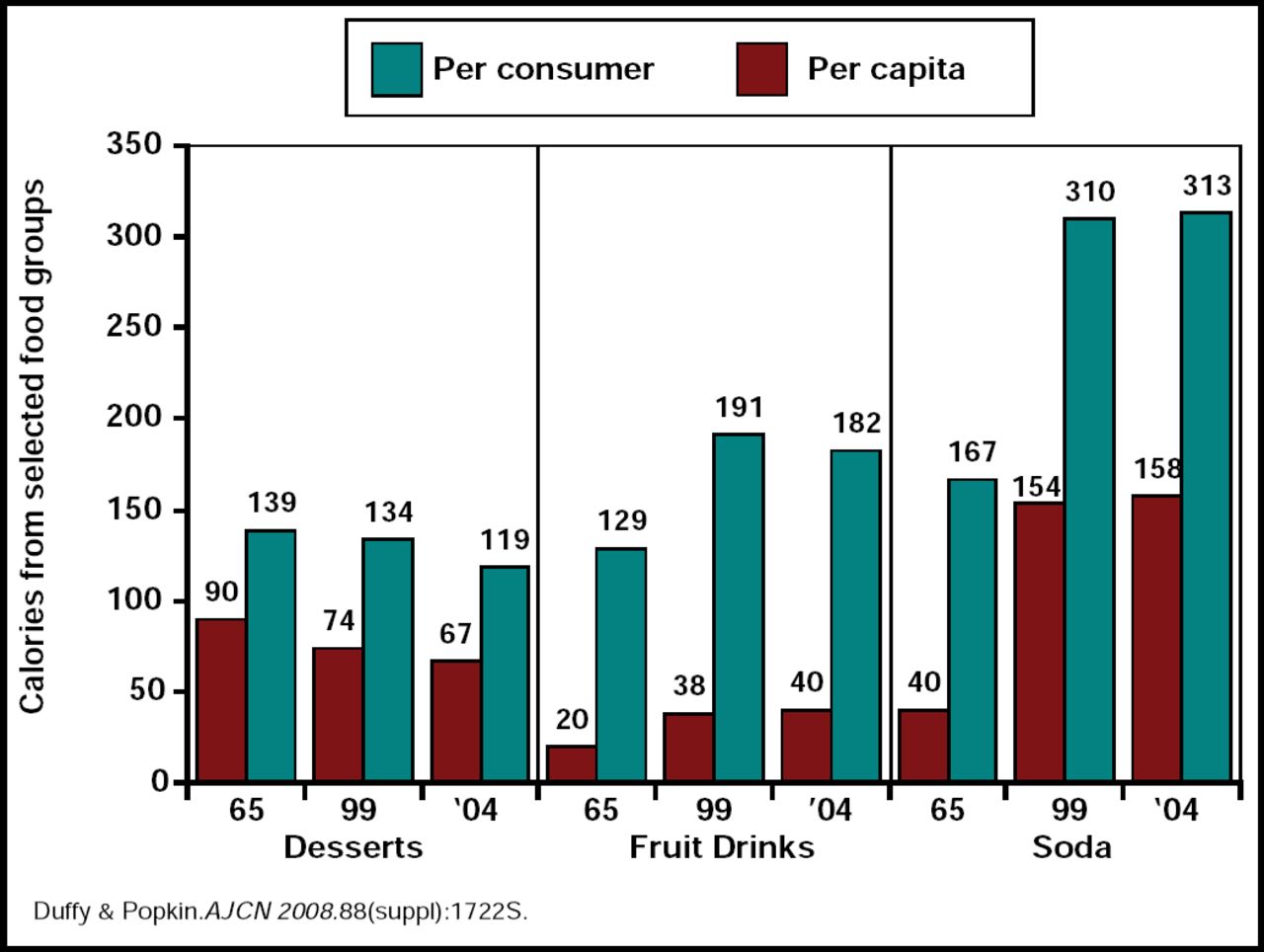
Barry Popkin, PhD, University of North Carolina, Chapel Hill, NC, highlighted the significant increase in the consumption of refined sugars across the globe over the past 20 years, noting that the main source of this increase has come from sugar-sweetened beverages, including soft drinks, fruit drinks, energy drinks, and vitamin and other functional beverage waters (Figure 1).

Steepest Increase in Calories of Added Sugar from Soda, per Capita and Consumer Estimates.
During this same time, there was little change in water consumption and essentially no reduction in food intake to compensate for these additional beverage-related calories [Duffey KJ & Popkin BM. Obesity 2007]. “This upward trend in the consumption of sugar-sweetened beverages, combined with an accelerated shift toward inactivity, poor diet, and obesity, presents a serious global public health threat,” Dr. Popkin said.
The upswing in the prevalence of obesity in the United States began around 1980, about the same time that high-fructose corn syrup was adopted as the sweetener of choice for soft drinks. “As the consumption of soft drinks increased, the intake of fructose from sucrose and high-fructose corn syrup also increased,” said George A. Bray, MD, Pennington Center, Baton Rouge, LA.
The deleterious effects of overconsumption of sugar-sweetened beverages are well documented. In a study that compared the metabolic effects of fructose in 16 healthy male and female subjects, short-term fructose overfeeding produced significant (p<0.05) increases in fasting triglyceride levels (71%), endogenous glucose production (12%), alanine aminotransferase concentration (38%), and fasting insulin concentrations (14%) in male subjects versus insignificant increases in female subjects [Couchepin C et al. Diab Care 2008]. Oral ingestion of fructose has also been shown to result in a significant (p<0.01) increase in blood pressure that is not gender-related [Brown CM et al. Am J Physiol Regulatory Integrative Comp Physiol 2008].
In overweight individuals, a diet that is high in sucrose versus one that is high in artificial sweeteners has been shown to produce increases in several markers of inflammation (Table 1) [Sorensen LB et al. Am J Clin Nutr 2005]. Of particular relevance to the metabolic syndrome, fructose appears to have a much greater effect on increases in visceral fat than other sugars [Stanhope KL et al. J Clin Invest 2009; Stanhope KL & Havel PJ. Curr Opin Lipidol 2008].
”During 1999 and 2000, regular soft drinks represented a surprising 7% of calories in the US diet,” said Frank B. Hu, MD, Harvard Medical School, Cambridge, MA. “That number has since increased to an estimated 9% to 10%.”
Changes in Concentrations of Inflammatory Markers Associated with Sugar-Sweetened Beverages.
Several large prospective cohort studies are currently underway to study the effects of diet and lifestyle on the development of chronic disease. Participants in these studies are contacted every 2 to 4 years using a validated dietary questionnaire. Biological and DNA samples are also collected to study the effect of diet and lifestyle on biochemical markers and the interaction between genes and diet on disease risk.
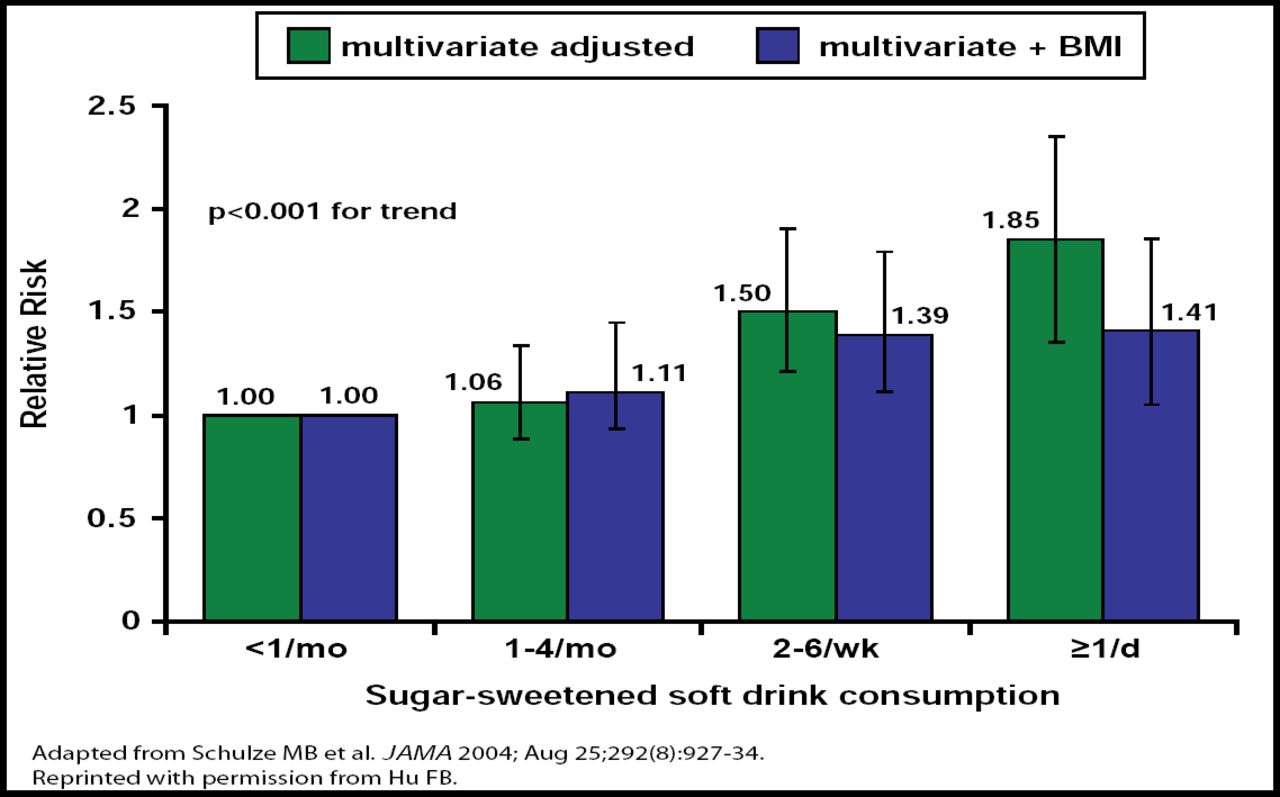
Eight-year data from the Nurses' Health Study II showed that individuals who increased their consumption of soft drinks during the first 5 years of the study and maintained a high level of consumption until the end of the study gained ∼8 kg, whereas individuals who had a relatively low level of consumption at baseline and maintained that level until the end of the study only gained 2 kg. Increased consumption of sugar-sweetened beverages was associated with a significant (p<0.001) trend for an increased risk of diabetes, regardless of whether the data were controlled for body mass index (BMI) [Schulze MB et al. JAMA 2004] (Figure 2). These results suggest that the detrimental effects of soft drinks on type 2 diabetes are not completely mediated through energy balance or body weight.

Sugar-Sweetened Soft Drinks and Type 2 Diabetes; Data from the Nurses' Health Study 2 for 1991–1998.
A similar association was identified for sugar-sweetened beverages and gestational diabetes (GDM) in this same cohort. “Women who consumed soft drinks regularly before pregnancy had more than a 20% increased risk of GDM,” said Dr. Hu, “with a slightly stronger association for sugar-sweetened cola versus other sugar-sweetened beverages.” Data from the Black Women's Health study also showed a significant relationship between sugar-sweetened soft drink consumption and the risk for diabetes [Palmer JR et al. Arch Int Med 2008]. Because of the increased risk of developing obesity and type 2 diabetes for African Americans, reducing caloric intake from sugar-sweetened soft drinks has a very important public health implication in reducing the health disparity for diabetes risk.
Recent data from the Framingham and Atherosclerosis Risk in Communities (ARIC) studies have identified a very strong association between soft drink consumption and the prevalence of the metabolic syndrome, as well as the risk of developing individual components of the metabolic syndrome. In the Framingham study, middle-aged adults who consumed at least 1 soft drink per day had a 44% higher adjusted risk (95% CI, 20% to 74%) of developing metabolic syndrome compared with those who consumed soft drinks infrequently [Dhingra R et al. Circulation 2007]. More recently, data from ARIC showed that diet soda intake, in particular, was strongly associated with an increased risk for the metabolic syndrome (HR, 1.34; 95% CI, 1.11 to 1.29) [Lutsey PL et al. Circulation 2008].
Other recent data from the Nurses' Health Study showed that regular soft drink consumption was associated with an almost 49% increase in risk of coronary heart disease in women, even after adjusting for BMI [Fung TT. Am J Clin Nutr 2009].
It is clear that the lack of food compensation when caloric beverages are consumed is one major cause of these health concerns. It is possible that an additional problem is the high glycemic load of sugar-sweetened soft drinks. Several mechanisms have been proposed, including evidence that high glycemic index/load diets lead to postprandial hyperglycemia, which in turn leads to hyperinsulimia and increased beta-cell demand. An alternative pathway may involve increased production of free fatty acids that leads to increased insulin resistance [Ludwig DS. JAMA 2002].
In summary, the symposium moderator called for an increased awareness of the role of sugar-sweetened beverages in precipitating metabolic syndrome. “Clearly, management of energy balance has become an issue. The evidence indicates that we need to be careful not only about the refined sugar in the foods we eat – but also in the beverages we drink.” said Jean Pierre Despres, Scientific Director, International Chair on Cardiometabolic Risk, Université Laval, Quebec, Canada.
The International Chair on Cardiometabolic Risk provides many free tools and resources to physicians and caregivers to support their management and education efforts with patients. For more information, visit www.cardiometabolic-risk.org.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.