

Summary
The consensus among presenters in this session was that although carotid endarterectomy (CEA) remains the most often used and the gold standard for treating carotid stenosis, 30-day stroke/death risks appear to be comparable between carotid artery stenting and CEA. This article discusses the NASCET, ESCT, and VA Trial, along with improvements in stenting outcomes and the need for aggressive treatment for transient ischemic attack.
- Interventional Techniques & Devices
- Cerebrovascular Disease
Management Strategies for the Asymptomatic and Symptomatic Patient with Carotid Stenosis
The consensus among presenters in this session was that although carotid endarterectomy (CEA) remains the most often used and the gold standard for treating carotid stenosis, 30-day stroke/death risks appear to be comparable between carotid artery stenting (CAS) and CEA.
Daniel Clair, MD, Cleveland Clinic Lerner College of Medicine, Cleveland, OH, reviewed the recent trials that have compared the use of CEA and CAS for the treatment of carotid stenosis. Introduced in the 1950s, the track record for CEA has been consistently improving, wherein the risks of major stroke or death are now in the low single digits.
Three trials—the North American Symptomatic Carotid Endarterectomy Trial (NASCET), the European Carotid Surgery Trial (ECST), and the Veterans Affairs (VA) Trial (stopped early)—have demonstrated the efficacy of CEA in symptomatic (transient ischemic attack [TIA], stroke) patients with a stenosis of the ipsilateral carotid artery. In these trials, combined death/stroke rates ranged from 5.5% to 7% in patients with stenosis of 70% to 99%, with an absolute benefit from CEA of 11.6% compared with the best medical treatment. Absolute risk reduction ranged from 7% to 17% up to 5 years later, indicating an obvious benefit for CEA. Stroke outcome risks were even lower in patients with asymptomatic stenosis (1% to 2%). Key factors that are associated with low death/stroke outcome rates are the preoperative use of antiplatelet drugs, the use of patch angioplasty, and the number of CEAs that the hospital/surgeon has performed.
CAS gained acceptance following the Stenting and Angioplasty with Protection of Patients with High Risk for Endarterectomy (SAPPHIRE) trial and its follow-up trial, SAPPHIRE WW. The SAPPHIRE trials were randomized studies that showed that CAS was not inferior to CEA in the treatment of high-surgical-risk patients (high risk was due to physiological reasons; eg, coexisting heart failure). Stroke, myocardial infarction (MI), and mortality rates at 1 year were 5.8%, 2.5%, and 7% in the stented patients compared with 7.7%, 8.1%, and 12.9% in the CEA-treated patients, respectively. Overall, outcomes were significantly lower in anatomical (eg, previous carotid endarterectomy) versus physiological at-risk patients (2.8% vs 4.9%; p=0.03).
Postmarketing trials demonstrated 30-day patient outcomes that were consistent with longstanding AHA guidelines for asymptomatic patients with a severe carotid stenosis. Dr. Clair concluded that stenting results appear to be at or near outcomes for CEA as they currently are being performed in the US. Results from the Carotid Endarterectomy versus Stenting Trial (CREST) will be important for confirming this statement.
William A. Gray, MD, Columbia University Medical Center, New York, NY, reported on the rapid improvements in outcomes with stenting over the last 4 to 5 years since device approval. Improved operator experience and better patient selection appear to be driving adverse event rates to new lows for both symptomatic and asymptomatic patients with stenosis. The protection devices are also likely to be critical to the safety of the procedure. Medicare now mandates that embolic devices be used during carotid stenting in order for patients to be eligible for Medicare coverage.
The early incidence of stroke and death that are associated with CAS has been dropping as operators gain more experience with the procedure and is now reported to be between 1.5% and 3% in most of the contemporary prospective audited experiences. A number of trials also have confirmed that CAS and CEA are equally effective for stroke prevention in the long term. Although somewhat controversial due to its high initial stroke rate in the CAS group, the EVA-3S (Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis) trial reported that after the early initial hazards (higher 30-day incidences for stroke and death with stenting), the outcomes for any ipsilateral stroke, any stroke, and any stroke or death are virtual parallel out to 4 years for the 2 treatment approaches and demonstrate the stroke prevention efficacy of both therapies. EVA-3S 30-day findings were countered, however, by the SPACE trial, which reported a rate of death or ipsilateral ischemic stroke from randomization to 30 days after the procedure of 6.84% with CAS and 6.34% with CEA (absolute difference 0.51%; 90% CI, 1.89% to 2.91%). This lack of acute outcome differences also was seen out to 2 years, thus confirming the EVA-3S finding of equivalent stroke prevention between stenting and surgery.
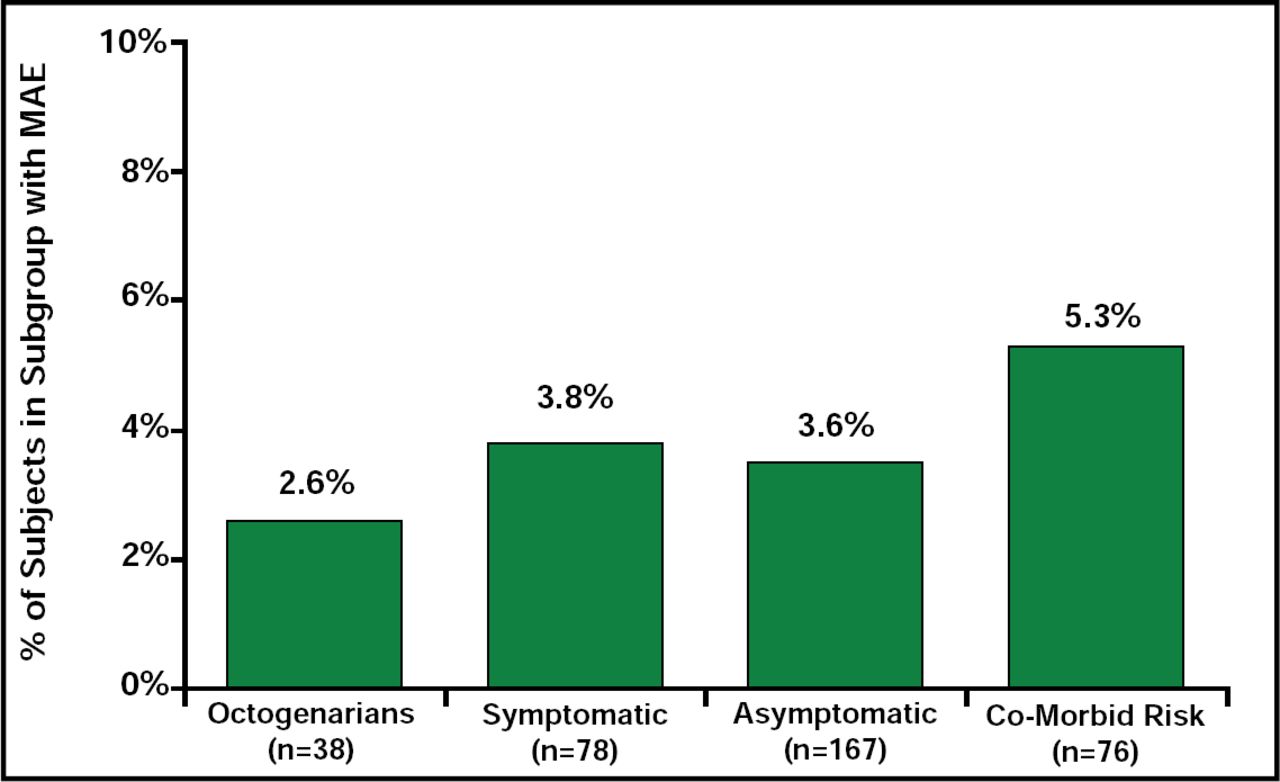
L. Nelson Hopkins, MD, University of Buffalo, Buffalo, NY, made a good case for treating, as well as enrolling into clinical trials, patients who are aged over 80 years with a high grade stenosis who are otherwise in good health. Recent data from The Gore EMPiRE Clinical Study indicated that stenting can lead to good results in octogenarians, with stroke, death, and MI rates as low as 2.6%. (Figure 1) In 2 other trials (CAPTURE II and EXACT), only 4.4% of the asymptomatic octogenarians experienced a stroke as a result of intervention, and this is a group that is normally at high risk for stroke.

EMPiRE Major Adverse Event Rates by Subgroup (Stroke, Death, MI).
Dr. Nelson's reasons for treating this patient group include the fact that stroke is the most expensive and devastating disease to treat, the risk of stroke increases dramatically with age, many studies show increasing numbers of older patients who are undergoing treatment, and finally, the baby boomers are coming. Thus, he recommends treating if life expectancy is >5 years and if treatment risk is low.
As to the choice of CEA or CAS, although both have been shown to be effective, Dr. Nelson believes that CES is a better procedure for the elderly, because there is more experience with this approach; also, many trials have shown it to be effective, while a few have shown a somewhat higher risk for CAS in the elderly. “Better patient selection and more experience will make the difference,” he concluded.
Joshua A. Beckman, MD, Brigham and Women's Hospital, Boston, MA, discussed the need to be aggressive with treatment for the patients who are having a TIA. He recommended immediate oral antiplatelet therapy over the use of an anticoagulant, because there is no evidence that anticoagulates work in this situation, and they increase the risk of bleeding. These medications should be started while the patient is still in the hospital, because there is a far greater rate of compliance compared with starting them at the first office visit.
“Treatment is required quickly after recognition of a TIA or small stroke to prevent a large stroke or the patient's death,” he said. The NASCET and ECST studies showed that the majority of risk reduction occurs in the first couple of weeks following revascularization. After 12 weeks, there does not appear to be any further significant benefit.
Management options include lifestyle modifications, medications that are known to decrease general stroke risk (antiplatelet agents, statins, antihypertensive agents), and procedural intervention. As far as whether to use CEA or CAS, Dr. Beckman suggested, “Go with the person who does this procedure the best.”

The editors would like to thank the many members of the American College of Cardiology presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.