

Summary
Results from the Surgical Treatment for Ischemic Heart Failure [STICH; NCT00023595] trial showed that adding surgical ventricular reconstruction to coronary artery bypass surgery does not provide additional clinical benefit in terms of improved mortality or decreased incidence of cardiac-related hospitalizations in subjects with heart failure and coronary artery disease.
- Interventional Techniques & Devices
- Heart Failure Clinical Trials
No Additional Benefit from Surgical Ventricular Reconstruction When Added to CABG
Results from the Surgical Treatment for Ischemic Heart Failure (STICH; NCT00023595) trial, presented by Robert H. Jones, MD, Duke University Medical Center, Durham, NC, showed that adding surgical ventricular reconstruction (SVR) to coronary artery bypass surgery (CABG) does not provide additional clinical benefit in terms of improved mortality or decreased incidence of cardiac-related hospitalizations in subjects with heart failure and coronary artery disease (CAD).
It has been suggested that a surgical approach to remodeling through left ventricular volume reduction might improve outcomes for patients with CAD and heart failure [Alfieri O et al. Am J Cardiol 2003]. SVR has been shown to reduce the left ventricular volume, increase ejection fraction, and improve ventricular function [Athanasuleas CL et al. J Am Coll Cardiol 2004]. The STICH study, the first multicenter randomized clinical trial to evaluate SVR, was designed to examine whether SVR, combined with CABG, decreases death or cardiac hospitalization compared with CABG alone.
The study included subjects with a left ventricular ejection fraction (LVEF) ≤35%, CAD that was amenable to CABG, and dominant akinesia or dyskinesia that was considered appropriate for SVR. Subjects were assigned to receive either CABG alone (n=499) or CABG + SVR (n=501). The study population was predominantly male (85%); mean age was 62 years. Multivessel CAD was present in 91% of subjects, 20% had stenosis of the left main coronary artery, and the median LVEF was 28%. Approximately 35% of subjects had diabetes. The primary study outcome was a composite of death from any cause and cardiac-related hospitalization. Secondary outcomes included death from any cause at 30 days, hospitalization for any cause and for cardiovascular causes, myocardial infarction (MI), and stroke.
Although subjects who received CABG + SVR experienced a significantly (p<0.001) greater reduction in end-systolic volume index (average 83 to 67 ml/m2) compared with those who received only CABG (average 82 to 77 ml/m2), this did not result in a clinical benefit in terms of all-cause mortality or cardiac-related hospitalization. During the 48-month follow-up period, 59% of subjects in the CABG-only group died or were hospitalized for cardiac-related causes compared with 58% of patients in the CABG + SVR group (HR, 0.99; 95% CI, 0.84 to 1.17; p=0.90).
Between baseline and the latest follow-up, angina symptoms (Canadian Cardiovascular Society criteria) improved by an average of 1.7 classes (p=0.84), and New York Heart Association (NYHA) functional class improved by an average of 1 class in both groups (p=0.70). Results on the 6-minute walk test also improved in both groups of subjects. Although low in both groups, there was no difference in the rate of stroke or acute MI.
The STICH investigators also examined whether the SVR procedure benefited patients through improved quality of life (QoL), reflected as either psychological well-being or better physical functioning. In addition, cost data were collected on 196 of 200 United States study subjects. Results of this portion of the study were presented by Daniel B. Mark, MD, Duke University Medical Center, Durham, NC.
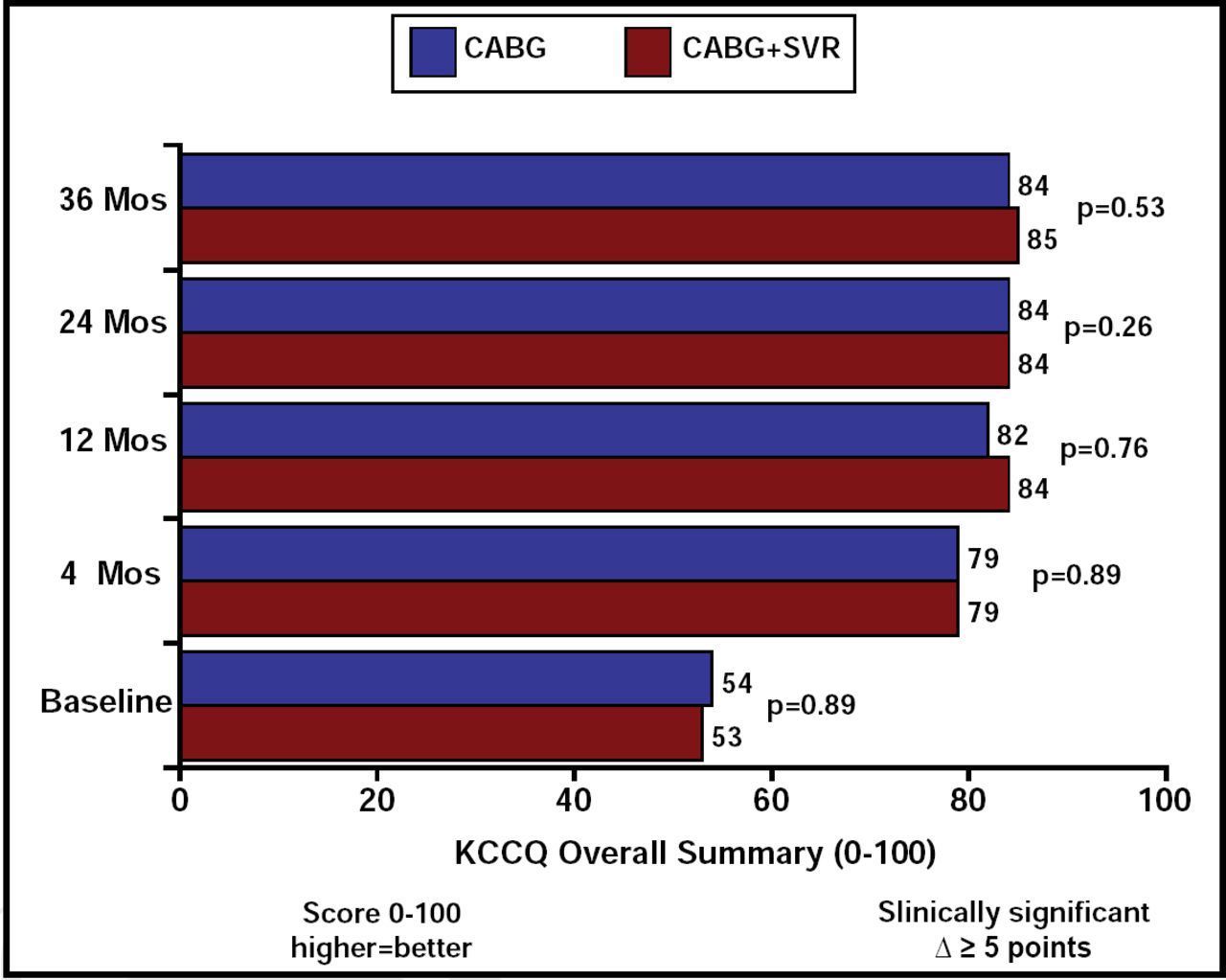
The primary QoL measure was the Kansas City Cardiomyopathy Questionnaire (KCCQ). Structured QoL interviews were conducted at baseline, 4, 12, 24, and 36 months postrandomization. Although both treatment groups significantly improved their KCCQ scores compared with baseline, the scores did not differ between the 2 treatment groups at any follow-up interval (Figure 1).

STICH QoL Substudy: KCCQ Overall Summary Score.
Operating times were longer for subjects in the combination group (5.5 hours vs 4.9 hours in the CABG-only group; p<0.001), as was the time on bypass (124 minutes vs 99 minutes in the CABG-only group; p<0.001). Subjects who received the combination surgery also required more postoperative care (eg, endocardial intubation and acute care) than subjects who received CABG alone. In a subset of United States patients who had cost information, the SVR procedure substantially increased the costs of the operation and postoperative care by an average of more than $14,500.
The investigators concluded that SVR is not justified in the population that was studied. Additional analyses are planned to determine if there are patient characteristics that may be associated with benefit or harm from adding SVR to CABG. The STICH study also has a second component that comprises subjects who were randomly assigned to receive either medical therapy alone or medical therapy plus CABG. This part of the study is ongoing.
“Our findings emphasize the importance of taking what appear to be medical breakthroughs and subjecting them to very rigorous comparisons with the best available therapy,” said Dr. Jones.
The clinical results of the STICH trial were published online in The New England Journal of Medicine on March 29, 2009. The QoL and economic analysis was published online in the American Heart Journal on March 30 2009.
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.