

Summary
Contrary to accepted wisdom, improvement in physical activity for stroke patients does not peak 11 weeks after being discharged from the hospital. This article presents data that detailed an exercise program that continues to improve fitness, walking, insulin sensitivity, and glucose metabolism in what he described as the chronic phase of stroke treatment.
- Cerebrovascular Disease
Contrary to accepted wisdom, improvement in physical activity for stroke patients does not peak 11 weeks after being discharged from the hospital. Richard F. Macko, MD, University of Maryland School of Medicine, Baltimore, MD, presented data that detailed an exercise program that continues to improve fitness, walking, insulin sensitivity, and glucose metabolism in what he described as the chronic phase of stroke treatment.
Community-based ambulatory activity profiles for patients in the chronic phase of hemiparetic stroke revealed that survivors demonstrated extremely low step counts and almost no step activity at high intensity (less than 3 minutes a day; Figure 1). The mean VO2 peak was associated with profound aerobic deconditioning and severe fatigue [Michael K. & Macko RF. Topics Stroke Rehabil 2007].

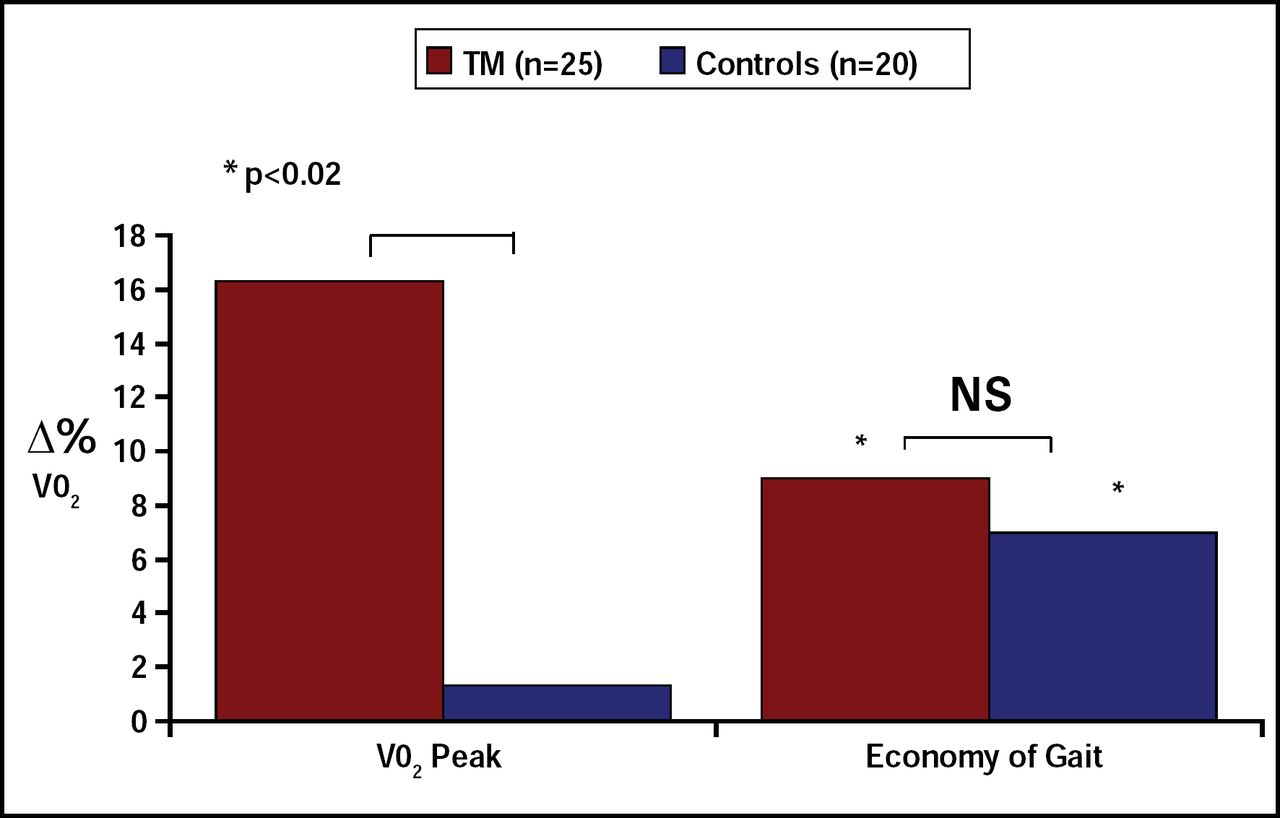
RESULTS: Effects of Treadmill Training on Fitness and Economy of Gait in Chronic Stroke.
In addition to inactivity, patients who survive stroke are predisposed to insulin resistance and glucose intolerance [Vermeer SE et al. Stroke 2006]. These risk factors can be amended with treadmill exercise training, which has been shown to reduce insulin resistance, improve glucose tolerance, and prevent diabetes in this patient group [Ivey FM et al. Stroke 2007].
The benefits of treadmill training (TM) were further examined in a 6-month progressive task-repetitive TM program in stroke patients with long-term mobility impairment. TM significantly improved (p<0.05) treadmill-walking velocity by 51% and cardiovascular fitness by 18% (p<0.05) compared with control subjects who were not in the program. Exercise-mediated improvements in walking velocity correlated with increased activation in the cerebellum and midbrain, the areas of the brain that are associated with motor activity [Ivey FM et al. Stroke 2007]. Higher-intensity levels of exercise produced better outcomes.
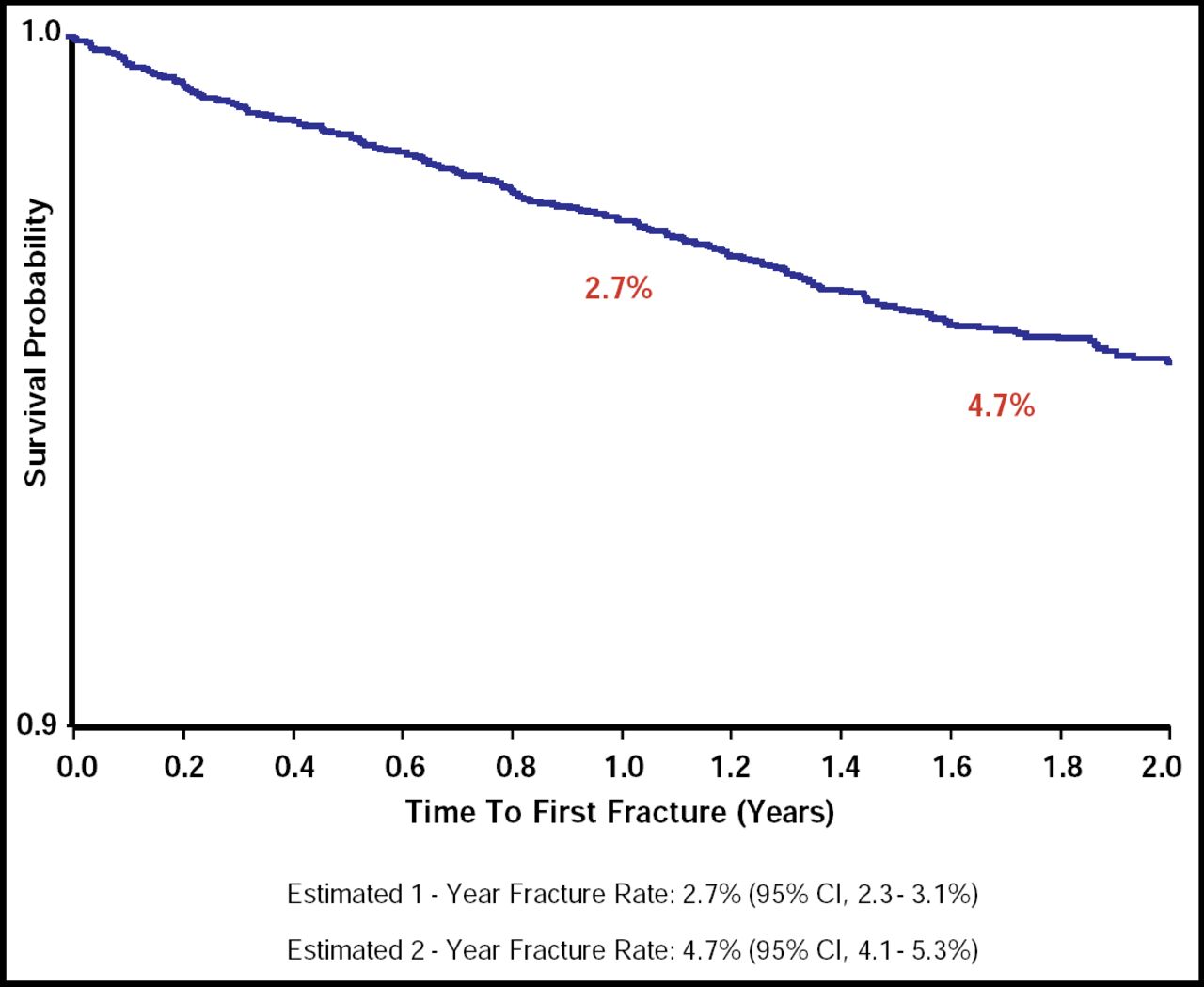
A comprehensive program that deals with the multiple aspects of chronic stroke recovery, including rehabilitation, transition, and community aspects, can improve cardiovascular function and endurance in survivors. Data indicate that patients who are released from postacute stroke rehabilitation programs experience impaired ambulation, decreased cardiovascular function, injuries from falls, and limited social participation. One study estimated that the 2-year fracture rates were 4.7% (95% CI, 4.1 to 5.3) for newly released stroke patients (Figure 2). Intermediate functional impairment conferred a higher fracture risk than mild or severe functional impairment [Whitson HE et al. J Am Geriatr Soc 2006].

2-Year Fracture Rates for Newly Released Stroke Patients.
Almost 50% of the community-dwelling stroke population needed full-time and able-bodied caregivers at home. A large proportion of these patients also reported depression, a lack of meaningful activity, and worsening of function. Further, data suggest a number of secondary problems: fewer than 50% of individuals with stroke have their risk factors assessed, treated, or controlled; 90% of those who are evaluated as overweight at initial evaluation remain overweight; only 51% of individuals who are hypertensive have their blood pressure under control; smokers do not quit smoking; and few participate in a exercise program.
“Evidence exists that extended home-based rehabilitation programs and physiotherapy improve functional independence following stroke. We need to do a better job of enrolling more patients into these programs,” concluded Pamela W. Duncan, PhD, Duke University, Durham, NC.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.