

Summary
This article reviews 2 studies that have used RNA as a biomarker for stroke and that exemplified the progress in and complexity of such studies, as well as discusses the potential use of biomarkers as predictors of stroke outcome and recovery.
- Cerebrovascular Disease Genomics
Frank Sharp, MD, University of California, Sacramento, CA, reviewed 2 studies that have used RNA as a biomarker for stroke and that exemplified the progress in and complexity of such studies.
“No single gene is a biomarker for stroke,” said Dr. Sharp. To illustrate this, he reviewed the results of a study that used RNA to characterize gene expression in peripheral white blood cells in subjects with acute ischemic stroke [Tang Y et al. J Cerebral Blood Flow Metab 2006]. Blood samples were taken < 3 hours following acute ischemic attack and again at Hours 5 and 24. By about 3 hours, ∼100 genes had changed, and by 5 and 24 hours changes were seen in ∼1000 genes, with a relatively few number of genes being shared at all time points. Using a mathematical program, the investigators identified 23 genes that are most predictive of stroke. In another study, the same investigators showed that RNA expression can be used to differentiate stroke subtype. In that study, they identified a specific group of genes that are expressed after stroke that can differentiate cardioembolic from atherosclerotic stroke [Xu H et al. J Cerebral Blood Flow Metab 2008]. Plans are underway to determine if these markers have any predictive value.
Moving to the other end of the stroke cycle, Larry B. Goldstein, MD, Duke University, Durham, NC, discussed the potential use of biomarkers as predictors of stroke outcome and recovery.
Adipocytokines are associated with a reduction in the inflammatory response and are known to be markers of endogenous vascular remodeling. Their levels are reduced with obesity, diabetes mellitus, hypertension, and coronary disease. Adipocytokine levels of <4 ug/mL have been shown to be independent predictors of 5-year mortality poststroke (93% mortality; OR, 5.2; 95% CI, 2.1 to 18.4; Efstathiou SP et al. Stroke 2005). Other potential biomarkers of the inflammatory response are subsets of T cells, such as CD4+CD28– cells, which produce high amounts of interferon-γ and are associated with tissue damage. Normally, they represent <5% of the CD4+ cell population. Higher levels of CD4+CD28– cells have been shown to correlate with an increased risk of stroke recurrence and death [Nadareishvili ZG et al. Neurology 2004].
Molecular and cellular changes also might offer biomarkers of functional outcome. Animal studies have shown that tissue matrix metalloproteinases (MMPs), which are upregulated after ischemia, have a dual nature. They are deleterious in acute stroke but beneficial during the poststroke recovery period [Zhao LR et al. Stroke 2007]. One human study, measuring MMP-9 levels relatively soon after stroke and infarct volume and NIHSS after 48 hours, showed good correlations between mean MMP levels and CT infarct volume and between mean MMP levels and later NIHSS [Montaner J et al. Stroke 2001]. The S-100 proteins constitute a family of dimeric calcium-binding proteins that are released from damaged glia into blood. In human ischemic stroke, peak S100-β levels have been shown to correlate with infarct volume and functional outcome [Foerch C et al. Arch Neurol 2005].
Dr. Goldstein cautioned, “While it's easy to become enamored with these potential new biomarkers and they may provide additional information to help with prediction, they are going to have to be incredibly good to make a difference when added to the predictions we can make with very simple markers that we can all get now.”
“If we pick our biomarkers effectively, we can improve clinical trial efficiency, facilitate novel trial design, and conceivably promote more effective, large, and streamlined trials. Some of the new technologies may also allow us to begin to estimate, on an individual basis, accurate predictors of risk, diagnosis, and prognosis,” said Bruce M. Coull, MD, University of Arizona, Tucson, AZ.
The use of a very precise biomarker that occurs early and that predicts a relationship to an outcome may make it possible to decrease the number of clinical trial participants and the duration of the trial and thus its cost. He cautioned, however, that usually there is not 1 single or even 1 cluster of biomarkers that accounts for the total pathophysiology of a disease and that biomarkers typically do not predict toxicity; thus, they should be used with caution in phase III trials.
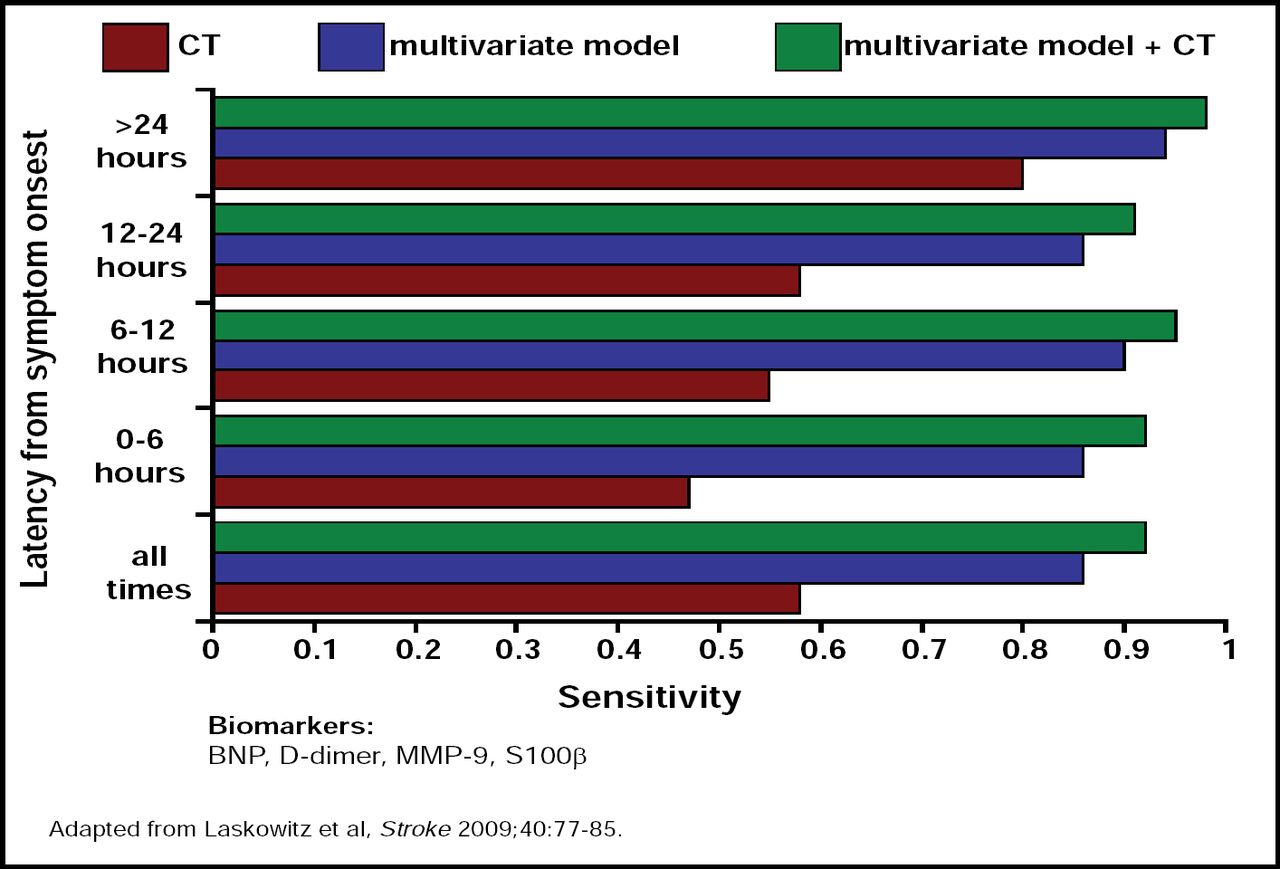
The complexity of the relationships between the biomarkers for stroke was well demonstrated in a recently published trial that showed that there were 4 biomarkers that were associated with acute stroke (BNP, d-Dimer, MMP-9, and S100-β; Table 1). While each was shown to have some relationship to the risk for acute stroke, their individual contributions were small. It was not until all 4 were present that the effect was identifiable [Laskowitz DT et al. Stroke 2009](Figure 1).
Potential Biomarkers for Use in Stroke Prevention.

Acute Stroke Test: Sensitivity of Initial CT and Biomarkers.
All of the speakers agreed that there is a need for continued development and recognition of biomarkers, particularly combinations of markers.
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.