

Summary
Despite technological advances and improved outcomes with percutaneous coronary intervention (PCI), treatment of chronic total occlusion (CTO) of coronary arteries remains a challenge. However, new techniques, such as retrograde wiring, have improved procedural success rates and clinical outcomes in patients who undergo PCI of a CTO. This article discusses data that support the use of PCI in patients with CTO and described different approaches to CTO PCI around the world.
- interventional techniques & devices
- coronary artery disease
Despite technological advances and improved outcomes with percutaneous coronary intervention (PCI), treatment of chronic total occlusion (CTO) of coronary arteries remains a challenge. However, new techniques, such as retrograde wiring, have improved procedural success rates and clinical outcomes in patients who undergo PCI of a CTO. In this session, presenters discussed data that support the use of PCI in patients with CTO and described different approaches to CTO PCI around the world.
Selecting Patients For CTO PCI
In this presentation, Jeffrey W. Moses, MD, Columbia University Medical Center, New York, NY, described his approach to selecting patients for CTO recanalization.
“In an environment of increased scrutiny of all PCI procedures, CTO treatment is under the microscope, and compelling clinical rationales are necessary,” said Dr. Moses. Still, the weight of evidence is in favor of aggressive treatment in many clinical scenarios, he added. For example, CTO PCI is an appropriate procedure for patients who require relief of exertional angina and other cardiovascular symptoms.
In a landmark observational study of 376 patients and 390 procedures, the procedural success rate for CTO PCI was 73.3%, and the incidence of complications was low (5.3%). After 1 year, patients with successful CTOs had a lower risk of cardiac death or myocardial infarction than those who had unsuccessful procedures (1.05% vs 7.23%; p=0.005). Patients who had successful CTO PCI were more frequently free from angina compared with those whose PCI was unsuccessful (88.7% vs 75.0%; p=0.008). This study suggests that CTO PCI is a feasible procedure that might be associated witih clinical benefits [Olivari Z et al. J Am Coll Cardiol 2003].
Recanalization of chronically occluded vessels might also improve ventricular function. In a study of 21 patients who underwent CTO PCI, both early and late improvements in regional left ventricular (LV) function were observed in the territory of the occluded vessel. Improvements were related to the extent of necrosis on pretreatment magnetic resonance imaging [Kirschbaum SW et al. Am J Cardiol 2008]
Persistent patency after CTO PCI improves long-term outcomes as well. In a single-institution trial of 847 consecutive patients, the CTO PCI procedural success rate was 65.1%. Compared with unsuccessful treatment, successful CTO PCI significantly reduced major adverse events (14.8% vs 5.5%; p<0.00001) and improved survival after 5 years (88.0% vs 93.5%; p=0.02). In this study, most events related to the need for repeat intervention [Hoye V et al. Eur Heart J 2005].
Based on current data and technology, the ideal candidate for CTO PCI has a single chronically occluded vessel that is solely responsible for the patient's symptoms or severe ischemia. With time and experience, clinicians can consider more challenging cases, such as patients with multiple CTOs. “Acquaintance and comfort with the technical possibilities allows clinical considerations to move to the forefront,” Dr. Moses concluded.
Japanese Approach To Chronic Total Occlusions
The Japanese experience with CTO PCI is considered a model of success by the EuroCTO Club and other groups. In this presentation, Masahiko Ochiai, MD, Showa University, Northern Yokohama Hospital, Kanagawa, Japan, and Dartmouth Medical College, Hanover, NH, described the evolution of CTO PCI use from the mid-1990s to present day in Japan.
In the mid-1990s, PCI devices included dedicated stiff wires that had excellent torque transmission, even inside the CTO. Procedures routinely involved the use of bilateral injections as well. In the late 1990s, physicians began using tapered stiff wires that had strong penetration power and good torque transmission. The parallel wire technique also gained popularity at that time.
Near the turn of the millennium, the concept of wiring changed dramatically, Dr. Ochiai said. In the new method, the wiring line is drawn prior to the procedure, and the operator advances dedicated stiff wires to follow the line precisely. “We noticed the impact of putting a radiopaque marker on the screen for precise wiring,” Dr. Ochiai said. “We do not rely on tactile feelings anymore. Instead, we look for objective findings to draw a precise wiring line,” he explained.
In the early 2000s, intravascular ultrasound (IVUS)-guided wiring was introduced. The most recent advance, introduced in the mid-2000s, was the use of preprocedure cardiac multislice computed tomography (MSCT; Figure 1).

Typical MSCT Image of Right Coronary Artery (RCA) Prior to Intervention.
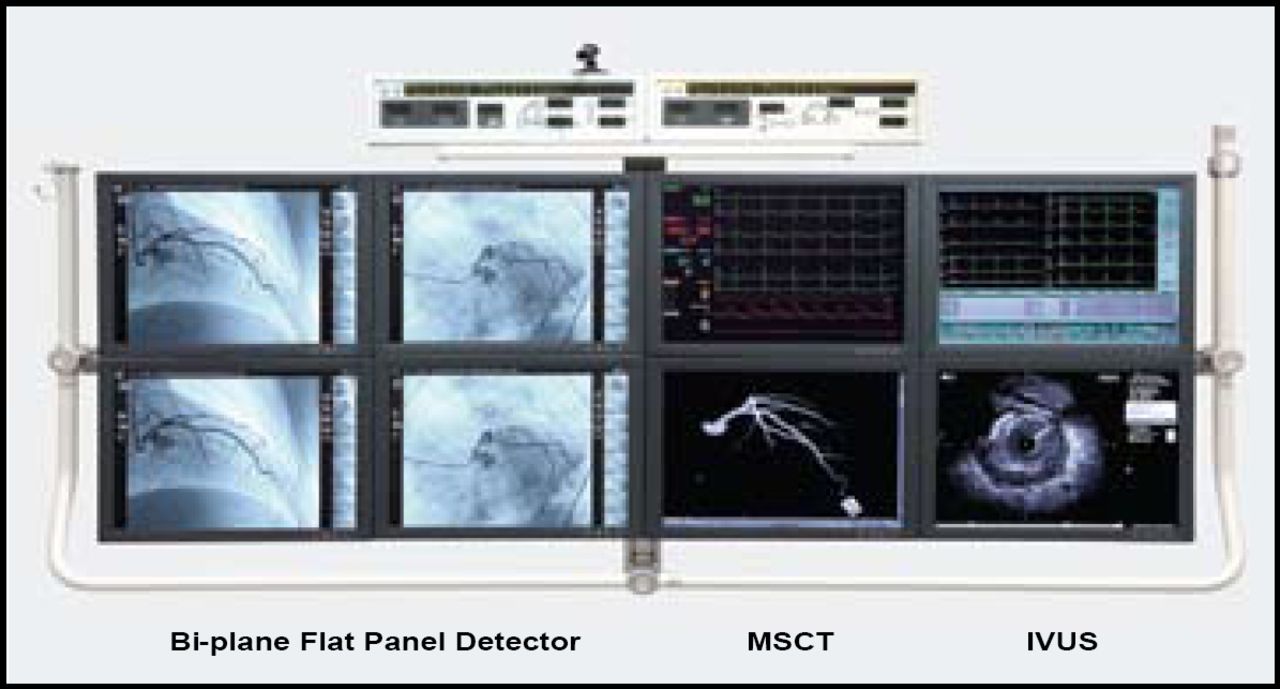
The integration of all imaging information, including MSCT, biplane flat panel detector imaging, and IVUS, is the key of procedural success, Dr. Ochiai said. He noted that the robust antegrade technique still is the most important and that the retrograde approach with a novel channel dilator will be a strong option for complex CTOs (Figure 2).

Monitors Installed in the Biplane Room of Dr. Ochiai's Cath Lab in Japan.
European Approach To CTOs
Carlo Di Mario, MD, PhD, Royal Brompton Hospital & Imperial College, London, UK, discussed the European approach to CTO management. In particular, he shared the highlights of a EuroCTO Club consensus paper, in which leading European interventionalists described best practices in the use of recanalization [Di Mario C et al. Euro Interv 2007].
Dr. Di Mario began by describing the optimal indications and strategies for CTO. According to the EuroCTO Club, decisions on the best treatment modalities for CTOs should stem from careful review of clinical history, results of sensitive provocative tests, coronary anatomy, and personal experience. In addition, ad hoc angioplasty is not recommended in the presence of CTOs, which needs proper procedure planning. With recanalization success rates that average better than 70%, the presence of a CTO should not be a sufficient reason to switch from PCI to surgery in multivessel disease.
Dr. Di Mario also described the EuroCTO Club's recommendations regarding CTO training and operator competency. The EuroCTO Club recommends that all interventional cardiology trainees acquire the theoretical knowledge to appropriately select candidates for CTO treatment and gain the practical experience to avoid the most common mistakes in CTO recanalization. Even after the recommended 2 years of training that is sufficient to work as an independent primary operator, a sensible operator should refrain from engaging in the recanalization of complex CTOs without appropriate supervision, the EuroClub guidelines state.
The EuroCTO Club suggests performing a minimum of 50 CTOs per year to maintain competency. This requirement translates into a model in which a limited number of operators and centers are allowed to perform CTO treatment, with selection based on workload and audited success and complication rates. “The interventionalist approaching CTO must handle complex techniques not required for normal lesion treatment, including the use of bilateral injection, parallel wires, stiff steerable dedicated wires, and the retrograde approach,” Dr. Di Mario said. Subspecialization is critical to reaching the success rates that are observed in Japan, he concluded.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.