

Summary
An early invasive strategy is as safe as delayed invasive management in patients with unstable angina or non-ST-segment elevation myocardial infarction (NSTEMI), according to findings from the Timing of Intervention in Patients with Acute Coronary Syndromes [TIMACS; NCT00552513] trial. However, early invasive care does not significantly reduce the risk of death, new myocardial infarction, or stroke compared with a delayed invasive strategy in most patients, except for those who are at the highest risk for adverse events.
- myocardial infarction clinical trials
- interventional techniques & devices
An early invasive strategy is as safe as delayed invasive management in patients with unstable angina or non-ST-segment elevation myocardial infarction (NSTEMI), according to findings from the TIMACS (Timing of Intervention in Patients with Acute Coronary Syndromes; NCT00552513) trial. However, early invasive care does not significantly reduce the risk of death, new myocardial infarction (MI), or stroke compared with a delayed invasive strategy in most patients, except for those who are at the highest risk for adverse events.
The TIMACS trial included 3031 patients who were randomly assigned to an early invasive strategy that included coronary angiography within 24 hours followed by percutaneous coronary intervention (PCI) or coronary artery bypass graft (CABG) as needed (n=1593), or to a delayed strategy in which patients received angiography, PCI, or CABG 36 hours or more after the onset of symptoms (n=1438). The median times to angiography in the early and delayed groups were 14 and 50 hours, respectively.
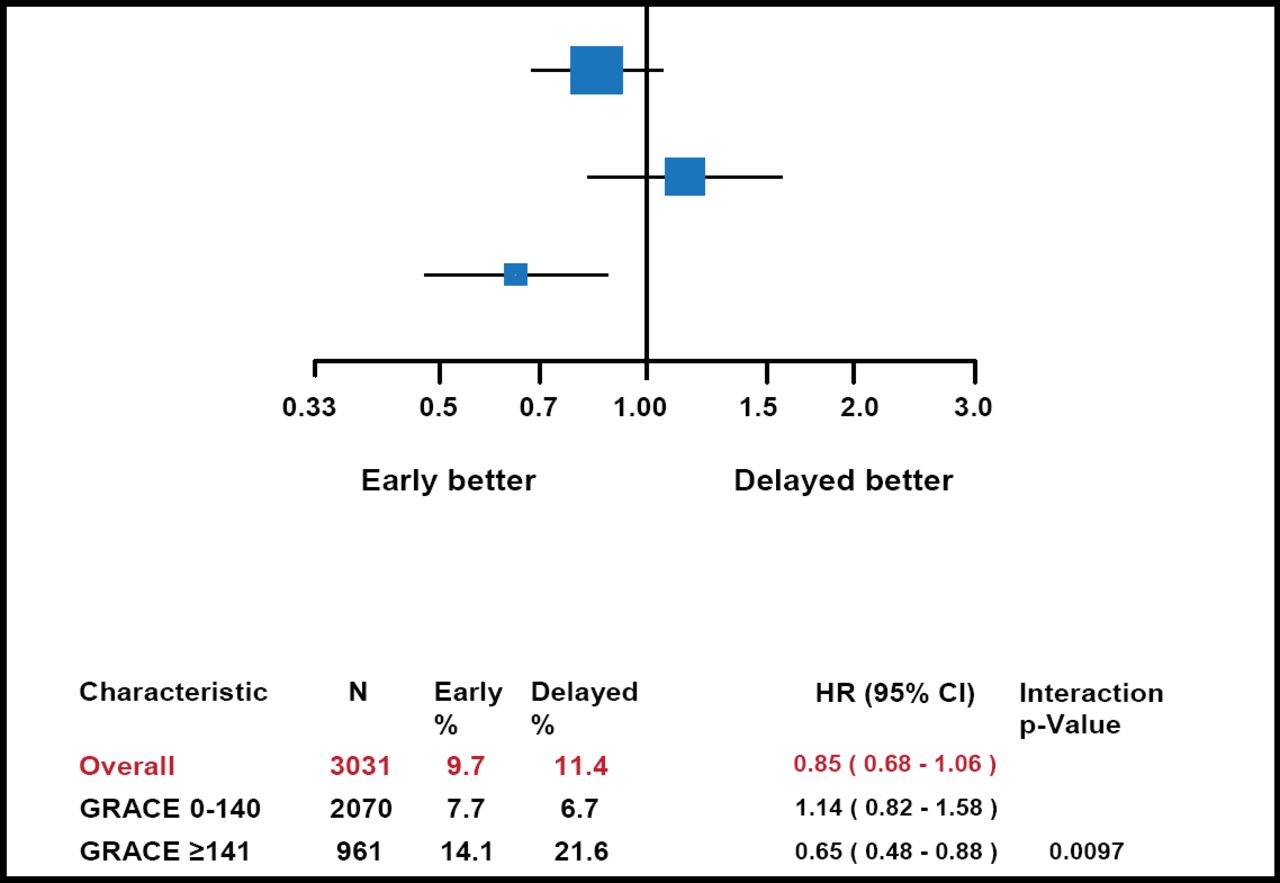
Patients in the early and delayed management groups had similar rates of the primary composite endpoint of death, MI, or stroke within 6 months (9.7% vs 11.4%, HR, 0.85; 95% CI, 0.68 to 1.06; p=0.15; Figure 1). In a secondary endpoint analysis, early invasive management reduced the risk of refractory ischemia compared with delayed management (1.0% vs 3.3%; HR, 0.30; 95% CI, 0.17 to 0.53; p<0.00001), without increasing the risk of major bleeding during the index hospitalization (3.1% vs 3.5%; p=0.53).

Primary Outcome of Death, MI, or Stroke at 180 Days.
Early management also reduced the risk of death or cardiovascular events among patients who were at high risk for adverse events, as determined by GRACE (Global Registry of Acute Coronary Events) scores ≥140. For patients with low or intermediate risk according to GRACE scoring, the 6-month risk of death, MI, or stroke was similar in the early and delayed management groups (7.7% vs 6.7%; p=0.43). However, among patients in the high-risk group, early management reduced this risk by 35% compared with delayed management (14.1% vs 21.6%; HR, 0.65; 95% CI, 0.48 to 0.88; p=0.005; Figure 2).

GRACE (Global Registry of Acute Coronary Events) Scores.
“Most patients with acute coronary syndromes can be managed safely with either an early or a delayed invasive strategy,” said Shamir R. Mehta, MD, MSc, McMaster University, Hamilton, Ontario, Canada, who reported the TIMACS findings. However, early intervention appears to be superior for high-risk patients, who should be considered for early heart catheterization, he said.
“In all other patients with acute coronary syndrome, the decision regarding timing of intervention can depend on other factors, such as catheterization laboratory availability, health care system, convenience and economic considerations,” Dr. Mehta concluded.
- © 2009 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.