

Summary
Results of the SEARCH [NCT00124072] trial did not show a significant clinical benefit with simvastatin 80 mg versus 20 mg and failed to find any cardiovascular benefit of large doses of folic acid.
- lipid disorders clinical trials
Results of the SEARCH (NCT00124072) trial did not show a significant clinical benefit with simvastatin 80 mg versus 20 mg and failed to find any cardiovascular benefit of large doses of folic acid.
Rory Collins, MD, University of Oxford, Oxford, UK, presented the SEARCH results at the American Heart Association meeting in New Orleans.
It is generally accepted that the use of statin therapy to lower low-density lipoprotein cholesterol (LDL-C) levels can reduce the risk of heart attack, stroke, or a revascularization procedure; however, there has been some uncertainty as to how intensively LDL-C levels should be lowered.
SEARCH was the largest randomized trial and had the longest follow-up of any study that directly assessed the efficacy and safety of more- versus less-intensive LDL-C-lowering. The primary study outcome was major vascular events (MVEs; defined as nonfatal myocardial infarction (MI), coronary/noncoronary revascularization, death from coronary heart disease, or stroke). The study population of SEARCH included 12,064 subjects (mean age 64 years; 10,012 men; 2052 women) with a prior history of MI for whom statin therapy was indicated. Mean LDL-C at baseline was 97 mg/dL (2.5 mmol/L). Subjects were randomly assigned to receive either the standard 20 mg/day dosage of simvastatin (n=6033) or 80 mg/day simvastatin (n=6031).
After a mean of 6.7 years of treatment, LDL-C was on average 14% (14 mg/dL; 0.35 mmol/L) lower in the 80 mg group versus those who received standard therapy. The reduction was associated with 6% fewer heart attacks, strokes, or revascularizations.
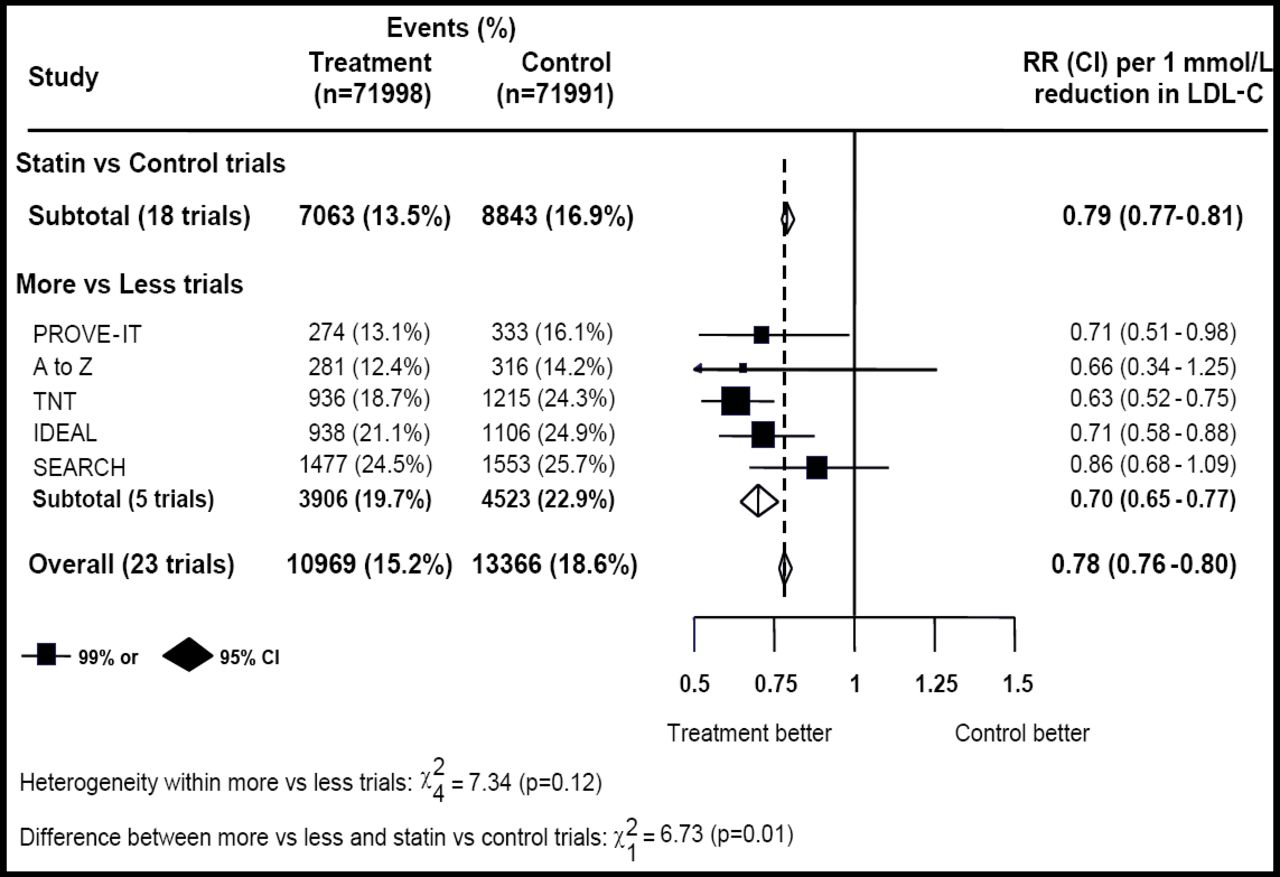
Although the difference between the 2 dosage groups was not significant, when the data from SEARCH were combined in a meta-analysis with data from 4 other studies of more versus less lipid-lowering [Cannon CP et al. N Engl J Med 2004; de Lemos JA et al. JAMA 2004; LaRosa JC et al. N Engl J Med 2005; Pedersen TR et al. JAMA 2005], lowering LDL-C further by an average of 20 mg/dL was shown to produce a 15% further reduction in MVE (Figure 1).

CTT Meta-Analysis: Effects of Statin on Major Vascular Event per mmol/L LDL-C Reduction.
The 80 mg/day simvastatin regimen was associated with a higher incidence of myopathy (53 cases vs 3 in the 20 mg dose group), 25 of which occurred in the first year.
A second objective of the SEARCH study was to evaluate the effect of folic acid on MVE. In a 2 × 2 factorial design, participants in SEARCH (none of whom had a clear indication for folic acid) also were randomly assigned to receive either 2 mg of folic acid + 1 mg of vitamin B12 daily (n=6033) or placebo (n=6031). The average homocysteine level at baseline was 13.5 μmol/L. After an average of 6.7 years of follow-up, although homocysteine levels were 3 to 4 μmol/L lower in patients who received the folic acid/vitamin combination, the reduction was not associated with a reduction in MVE (25.5% vs 24.8%; HR, 1.04; 95% CI, 0.95–1.14; p>0.05). Long-term supplementation with these vitamins was shown to be safe, however, with no significant excess of any major adverse events, including cancer.
Additional information on SEARCH can be found at http://www.searchinfo.org .
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.