

Summary
This article not only discusses the best treatment option for diagnosed type 2 diabetes mellitus (T2DM), but also the most prudent ways to prevent the onset of diabetes including managing at-risk individuals who (at present) only show evidence of impaired glucose tolerance, insulin resistance, or beta-cell function — so-called “prediabetics.”
- prevention & screening
- endocrinology
- diabetes mellitus
At issue is not necessarily the best treatment option for diagnosed type 2 diabetes mellitus (T2DM) but the most prudent way to prevent the onset of diabetes; managing at-risk individuals who, at present, only show evidence of impaired glucose tolerance, insulin resistance, or beta-cell function – so-called “prediabetics.”
Take a Pill
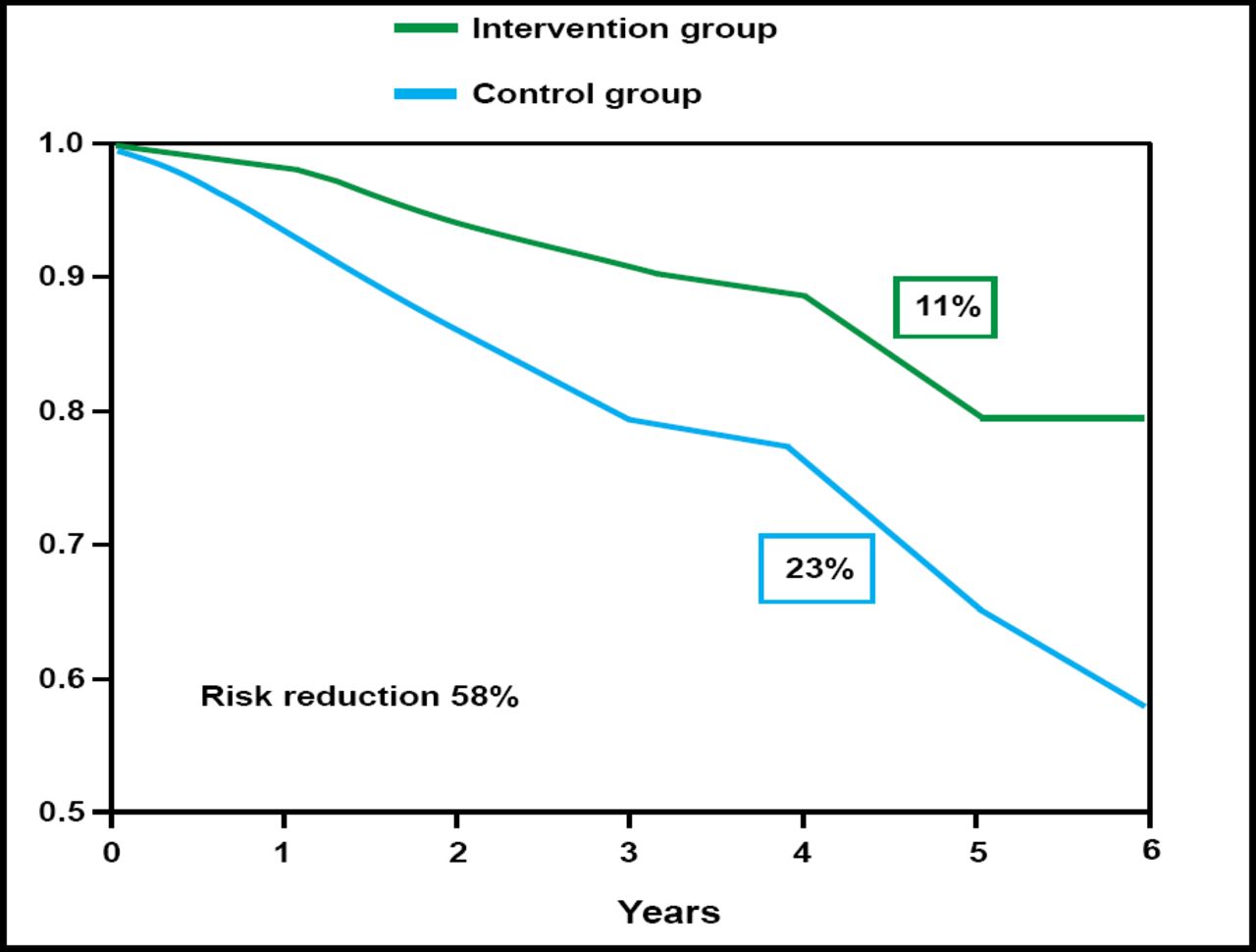
Large-scale initiatives that use lifestyle modification in a prediabetic population have been attempted, and results are encouraging. The Finnish Diabetes Prevention Study recorded a 58% reduction in risk for the intervention at 6 years, relative to the control group (Figure 1). “But at what cost?” asked Paul Zimmet, MD, PhD, Baker IDI Heart and Diabetes Institute, Melbourne, Australia. The Finnish lifestyle cohort required 7 nutritionist sessions in the first year, and one every 3 months thereafter. Patients were offered individualized guidance on physical activity and were engaged in this and other types of counseling for an average of 150 minutes/week. The Diabetes Prevention Program in the United States employs a similar expenditure of resources (with similar success).

Diabetes Development During Lifestyle Intervention: DPS Finland.
The tremendous costs of these intensive lifestyle programs aside, it still is an open question as to whether all lifestyle programs actually work. A recent paper that looked at this issue concluded that “a facilitated theory-based behavioral intervention was no more effective than an advice leaflet for promotion of physical activity” and that true, lasting change in individual lifestyle was unlikely to occur under current societal conditions (Kinmonth et al. Lancet 2008).
Reflecting this lack of faith in behavioral interventions are the American Diabetes Association's recently published treatment guidelines for patients with impaired fasting glucose and impaired glucose tolerance, which recommend lifestyle modification or metformin (Nathan et al. Diabetes Care 2007). “This is a basic rejection of the idea that lifestyle alone works,” said Dr. Zimmet. On the surface, the approach seems sound, but many individuals cannot or will not avail themselves of such a program; patients may be disabled; suffer from other chronic conditions, such as psychiatric disorders; have cultural or economic impediments to proper diet and exercise; or simply not have physical access to care.
In contrast, pharmacotherapy, easily obtained and simply administered, has been shown in numerous studies to be effective in the prevention of T2DM; these include the US DPP, STOP NIDDM, Xendos, and DREAM trials. In DREAM, treatment with rosiglitazone resulted in a 60% relative risk reduction for the prevention of diabetes as compared with placebo at 4 years (p<0.01); although no real impact on mortality has been shown.
Research has shown that microvascular complications occur well before a patient gains the artificial threshold of metabolic measures called “diabetes.” Evidence that lifestyle intervention reduces the incidence of cardiovascular disease (CVD) is scarce, but ample evidence does exist for the reduction of CVD with drug therapy in prediabetes. STOP-NIDDM showed a 49% reduction in CVD with acarbose (Chiasson et al. JAMA 2004).
“The real issue for me is not prevention of type 2 diabetes,” said Dr. Zimmet. “It's preventing the cardiovascular disease in people who get type 2 diabetes – that's the major cause of morbidity and mortality.”
Take a Hike
“Adverse lifestyle factors are the root cause of the current epidemic of T2DM,” began Nick Wareham, MD, PhD, MRC Epidemiology Unit, Institute of Metabolic Science, Cambridge, UK. Individually focused lifestyle changes are demonstrably effective in reducing progression to diabetes. A meta-analysis by Gillies et al. (BMJ 2007) consistently showed a halving of risk of progression to diabetes with changed behavior among high-risk individuals. “The point from our own ProActive study (Kinmonth et al. Lancet 2008) is not that lifestyle programs don't work but rather that this detailed behavioral approach was no more successful than simple advice.”
With lifestyle intervention, cost is relative. In terms of quality-adjusted life-years (QALYs), lifestyle change costs $31,512 per QALY versus $99,611 for metformin over the course of a clinical trial and, projected over a lifetime, amounts to $1100 per QALY for lifestyle and $31,300 for metformin (Herman et al. Annals of Internal Med 2005). If the intervention begins at the early ages of 25 to 44, lifestyle change actually is cost-saving to society. “There are few interventions in medicine that I can think of that are actually cost saving,” said Dr. Wareham, “so we are dealing with interventions that are cost-beneficial rather than just cost-effective.”
The pharmacological benefits to diabetes prevention only last as long as the duration of the drug treatment, and people revert to the same risk as those in the placebo group when the drug is discontinued. In contrast, the benefits of lifestyle intervention are prolonged. This effect was shown to be very long-term by Li et al., who published 20-year follow-up data from the Da Qing intervention study (Lancet 2008).
“Although we would ideally want long-term data from behavioral trials with clinical endpoints such as cardiovascular events, these are difficult to conduct and have so far not been undertaken,” Dr. Wareham said. The Da Qing study did demonstrate a favorable impact on cardiovascular risk, but this was not statistically significant because the study was relatively small. “Given the importance of these issues for public health, we would hope that funders would acknowledge the need for large randomized controlled trials to address this issue in the future,” commented Dr. Wareham. In contrast to drugs, which only tend to impact a single risk factor, there is a clear argument for additional benefits of lifestyle interventions or “halo effects,” which translate as improvements in physical, mental, and social function that are included in the concept of general well-being. The assessment of general health –how you feel about your health – is a strong predictor of all-cause mortality and was modified favorably by the physical activity intervention in the ProActive study.
Dr. Wareham also questioned the level of evidence that is required to start pharmacological therapy for people who are at risk for a disease to prevent a condition from arising in the future. Because these people are not patients, but are offered preventive treatments on the basis of their risk profile, he argued that the level of evidence should be high. “One would question the wisdom of basing our policy decisions on assumptions,” Dr. Wareham added. Although data from highly publicized trials like DREAM show that pharmacological intervention can reduce risk of progression to diabetes by 60%, this really is a proxy intermediate outcome. The data from these studies on prevention of cardiovascular outcomes are far less impressive, which perhaps is not surprising because glucose is not a particularly strong cardiovascular risk factor. Even if one could achieve the level of CVD risk that is predicted from observational data (Levitan et al. Arch Int Med 2004), then glucose-lowering alone would be a poor individual therapeutic strategy, because the predicted absolute risk reduction would not be great and the number that is needed to treat for 3 years to prevent one cardiovascular event would be high at 554.
Given that the behavior issues that drive the current obesity and diabetes epidemics are societal issues, the only appropriate strategy that meaningfully impacts this public health problem is to move away from focusing on high-risk strategies. Instead we need to concentrate on understanding the determinants of the population distribution of behaviors and on public policy approaches to trying to move that distribution in a favorable direction. Dr. Wareham concluded, “Public health problems require public health solutions,” and these require a considerable scaling-up of investment in public health research to underpin those solutions.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.