

Summary
Insulin resistance is emerging as a major contributor to cardiovascular risk, and the lipotoxicity that is associated with obesity is a key factor in the development of insulin resistance. Recent data that suggest that thiazolidinediones may provide some insight into this issue are reviewed in this article.
- diabetes mellitus
- cardiometabolic disorder
- insulin
- lipid disorders
- obesity
- endocrinology
Insulin resistance is emerging as a major contributor to cardiovascular risk, and the lipotoxicity that is associated with obesity is a key factor in the development of insulin resistance (IR). Recent data that suggest that thiazolidinediones (TZDs) may provide some insight into this issue were reviewed by Ralph A. DeFronzo, MD, University of Texas Health Science Center, San Antonio, TX.
Insulin resistance is a characteristic of type 2 diabetes mellitus (T2DM) and all components of the metabolic syndrome. Macrovascular disease (myocardial infarction [MI], stroke) accounts for 80% of all mortality in T2DM. So, how large a role does hyperglycemia play in the pathogenesis of atherosclerosis in diabetic subjects, and does glycemic control alone improve cardiovascular disease (CVD) outcome?
A report from the UK Prospective Diabetes Study showed a 37% reduction in microvascular events (retinopathy, neuropathy), a 12% decrease in stroke, and a 14% reduction in MI per 1% reduction in HbA1c levels (Stratton. BMJ 2000). However, these results have not been replicated in the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) or the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trials. This result may be explained by an incorrect hypothesis, the wrong patient population (already exhibiting cardiovascular damage due to long-term diabetes), or an inadequate sample size. In order to sufficiently power a trial that could determine if glycemic control alone reduces CVD risk, approximately 6800 patients would be required to participate in a 10-year study.
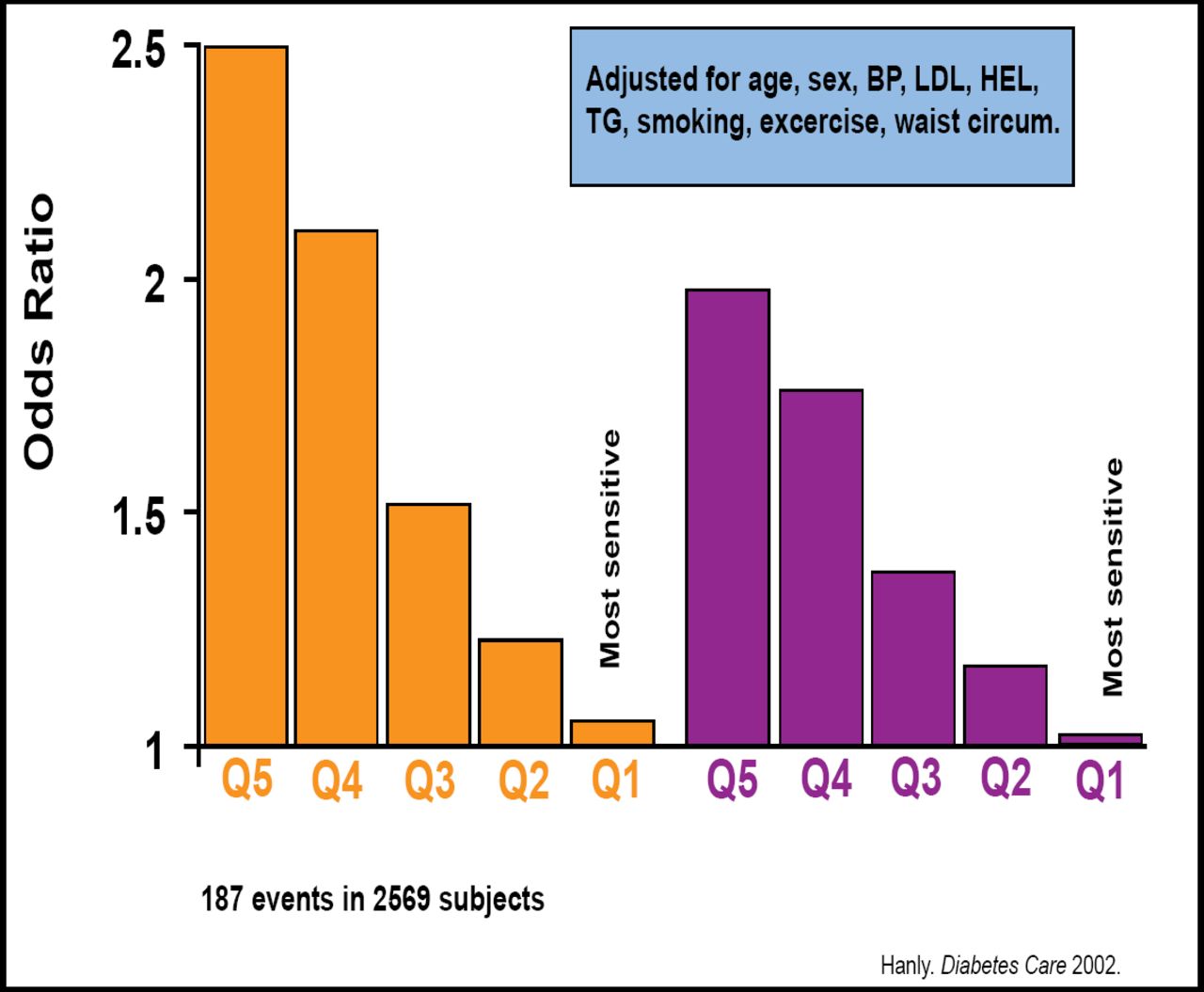
Despite this lack of direct evidence, multiple prospective epidemiological studies have demonstrated that both IR and the metabolic syndrome are predictive of CVD as well as future diabetes onset. In the San Antonio Heart Study (SAHS), after adjusting for age, gender, high cholesterol, and smoking status, IR is indicated as a predictor of CVD development in nondiabetic patients at an 8-year follow-up (Hanly et al. Diabetes Care 2002; Figure 1).

Association Between HOMA-IR and 8-Year Incidence of CVD in Nondiabetic Subjects in SAHS.
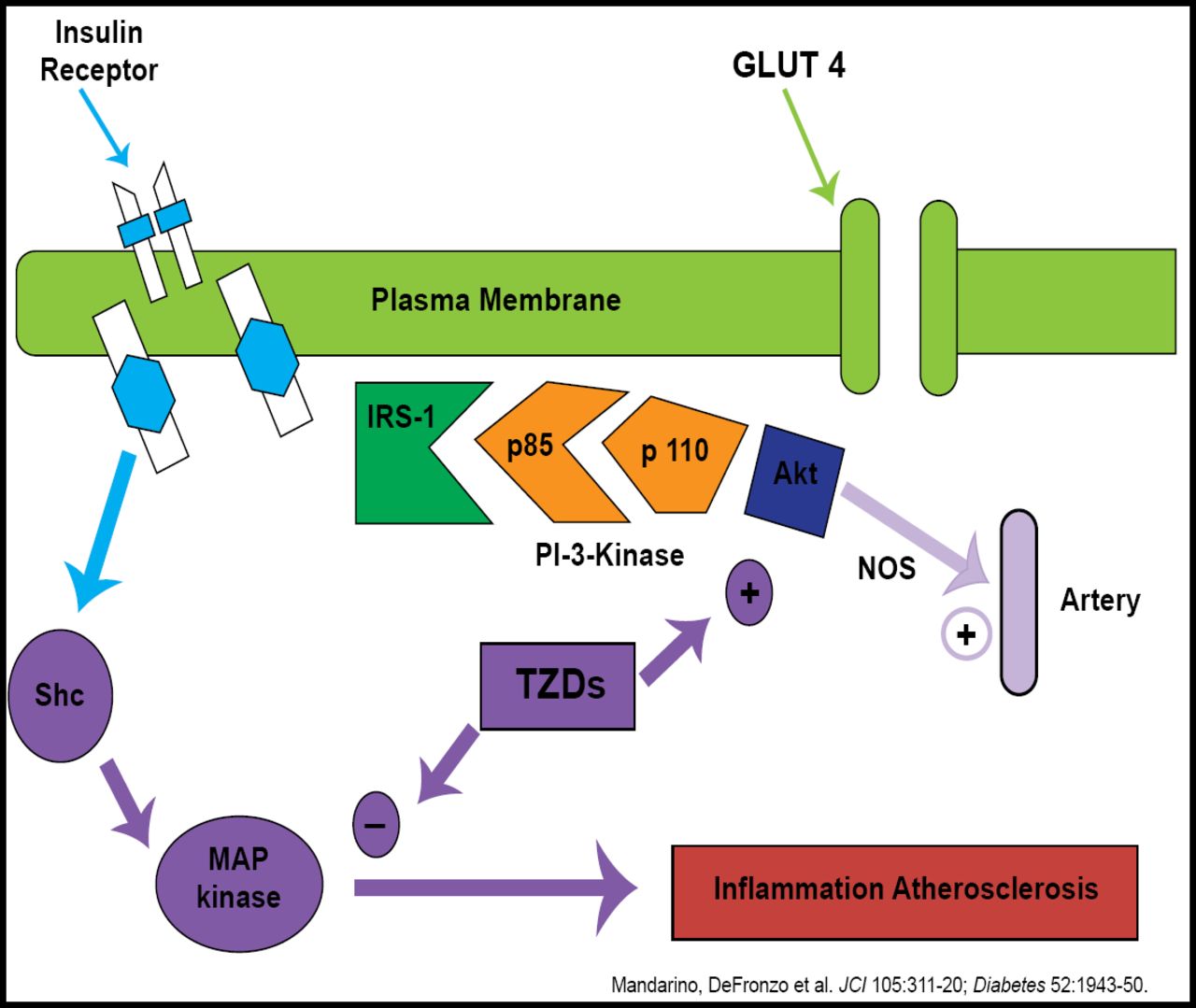
Data from numerous laboratories recently have elucidated the pathways that account for IR and its impact on CVD risk. In brief, insulin receptor substrate-1 (IRS-1) is the initial transmitter of the insulin signal at the cell membrane. Once it is activated, this molecule can then go on to promote not only glucose metabolism but also vasodilation via the PI-3 kinase pathway. Alternately, under conditions of IR, IRS-1 can induce MAP kinase activation, leading to the inflammation that is characteristic of the formation of atherosclerosis (Mandarino et al. Diabetes 2003).
Given the dual nature of IRS-1 signaling, it is not feasible to block its activity with a drug – the loss of the PI-3 pathway would negate any benefit that is derived from shutting down MAP kinase. However, the TZD drug class hits both targets and is able to stem inflammation that is caused by IR while at the same time facilitate arterial well-being via PI-3 kinase/NOS signaling (Figure 2; DeFronzo et al. Diabetes 2003).

Insulin Signal Transduction System in T2DM Humans: Effect of TZDs.
The TZDs also can address lipotoxicity, a factor that also is shown to drive CVD risk (Kashyap Diabetes 2003). Operating through the NF-kappa B pathway, free fatty acids (FFAs) induce inflammatory cytokines while at the same time downregulate the beneficial PI-3 pathway. In several studies of TZD, pioglitazone has been shown to reduce FFA and reduce cardiovascular events in T2DM subjects (PROactive Investigators. Lancet 2005). There also is evidence to show that pioglitazone halts the progression of atherosclerosis (Nissen. JAMA 2008).
Together, these observations argue for a greater emphasis on the treatment of IR and the management of prediabetic obese patients.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.