

Summary
Interventions that are designed to lower blood pressure or increase glucose control both improve outcomes in patients with type 2 diabetes mellitus. Together, these strategies provide even greater protection against diabetes-related complications, according to new findings from the Action in Diabetes and Vascular Disease [ADVANCE] trial.
- diabetes mellitus
- diabetes & endocrinology clinical trials
- endocrinology
- hypertensive disease
Interventions that are designed to lower blood pressure or increase glucose control both improve outcomes in patients with type 2 diabetes mellitus (T2DM). Together, these strategies provide even greater protection against diabetes-related complications, according to new findings from the Action in Diabetes and Vascular Disease (ADVANCE) trial.
In the ADVANCE trial (NCT00145925), 11,140 patients with T2DM were randomly assigned to treatment with a fixed-dose combination of perindopril and indapamide or placebo for blood pressure control, and to either intensive glucose-lowering with gliclazide or standard guideline-based therapy. The main results have been reported previously from the blood pressure-lowering arm (ADVANCE Collaborative Group. Lancet 2007) and glucose control arm (ADVANCE Collaborative Group. N Engl J Med 2008). In the current presentation, John Chalmers, MD, University of Sydney, Sydney, Australia, reported additional findings that were related to each intervention and discussed the joint effects of both blood pressure control and intensive glucose control.
Blood Pressure-Lowering
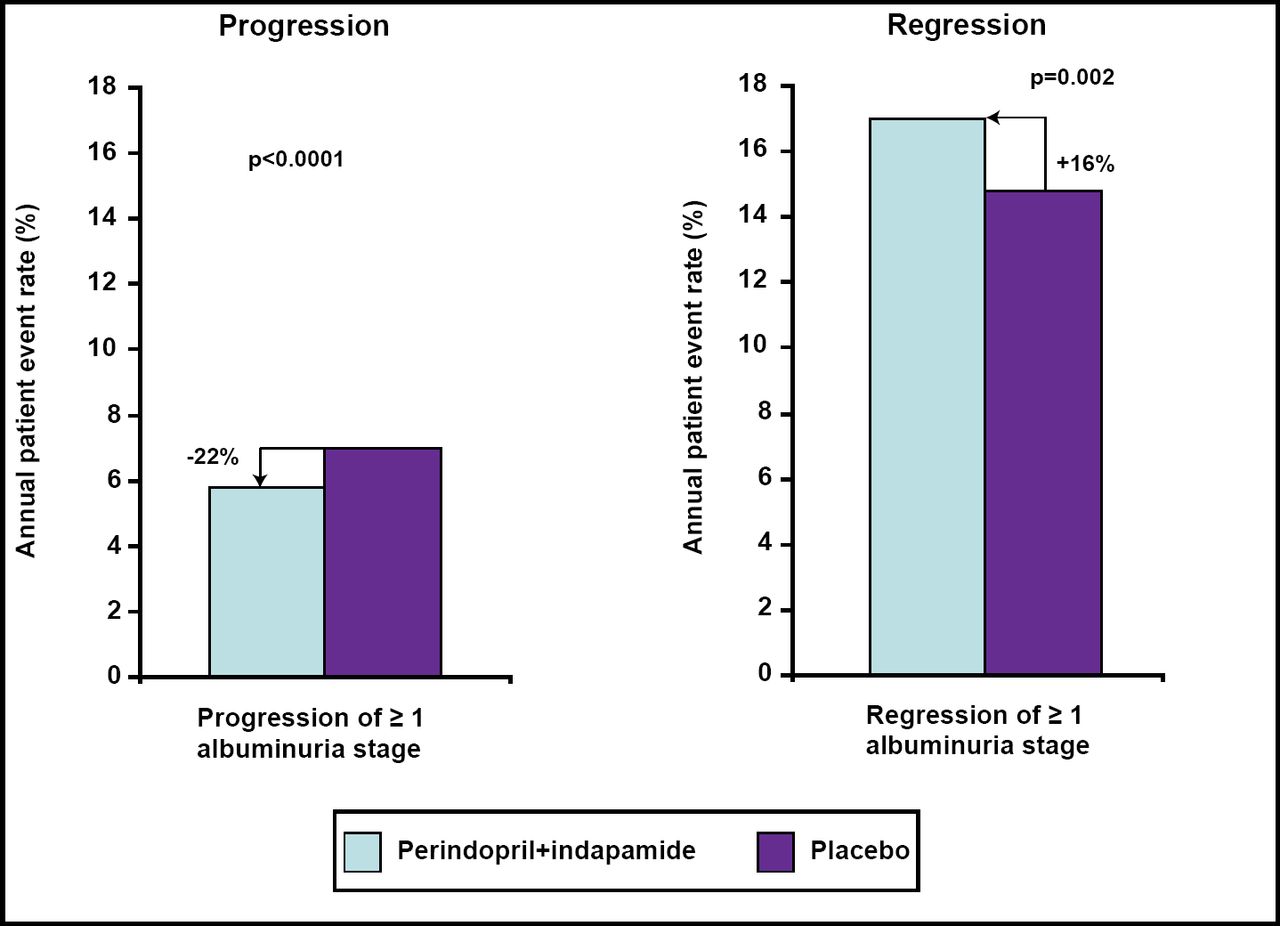
Compared with placebo, the combination of perindopril and indapamide reduced the risk of several outcomes, including all-cause mortality (14%), cardiovascular death (18%), major vascular events (9%), total coronary events (14%), and total renal events (21%). A closer examination of renal outcomes showed that perindopril and indapamide reduced the progression of albuminuria by 22% and increased the regression of albuminuria by 16% compared with placebo (Figure 1).

Blood Pressure Control and Albuminuria.
Findings from this arm of ADVANCE support the recommendations of current guidelines for lower blood pressure targets (<130/80 mm Hg) in patients with T2DM, Prof. Chalmers said. They also confirm that blood pressure should be lowered routinely in all patients with T2DM, regardless of initial blood pressure levels, he added.
Intensive Glucose Control
Patients who were treated with intensive glucose control had a lower mean HbA1c (6.5%) at the final visit in the ADVANCE trial than those who were treated with standard therapy (7.3%; p<0.001). In addition, compared with guideline-based strategy, intensive glucose-lowering therapy prevented major microvascular events (HR=0.86; p=0.01) and diabetic nephropathy (HR=0.79; p=0.006).
“Treatment with a pragmatic and progressive glucose control regimen, as used in ADVANCE, can help patients to achieve an HbA1c of ≤6.5% and reduce serious complications, especially renal events,” Prof. Chalmers said. Intensive therapy was associated with acceptable rates of hypoglycemia and no evidence of weight gain.
Joint Effects
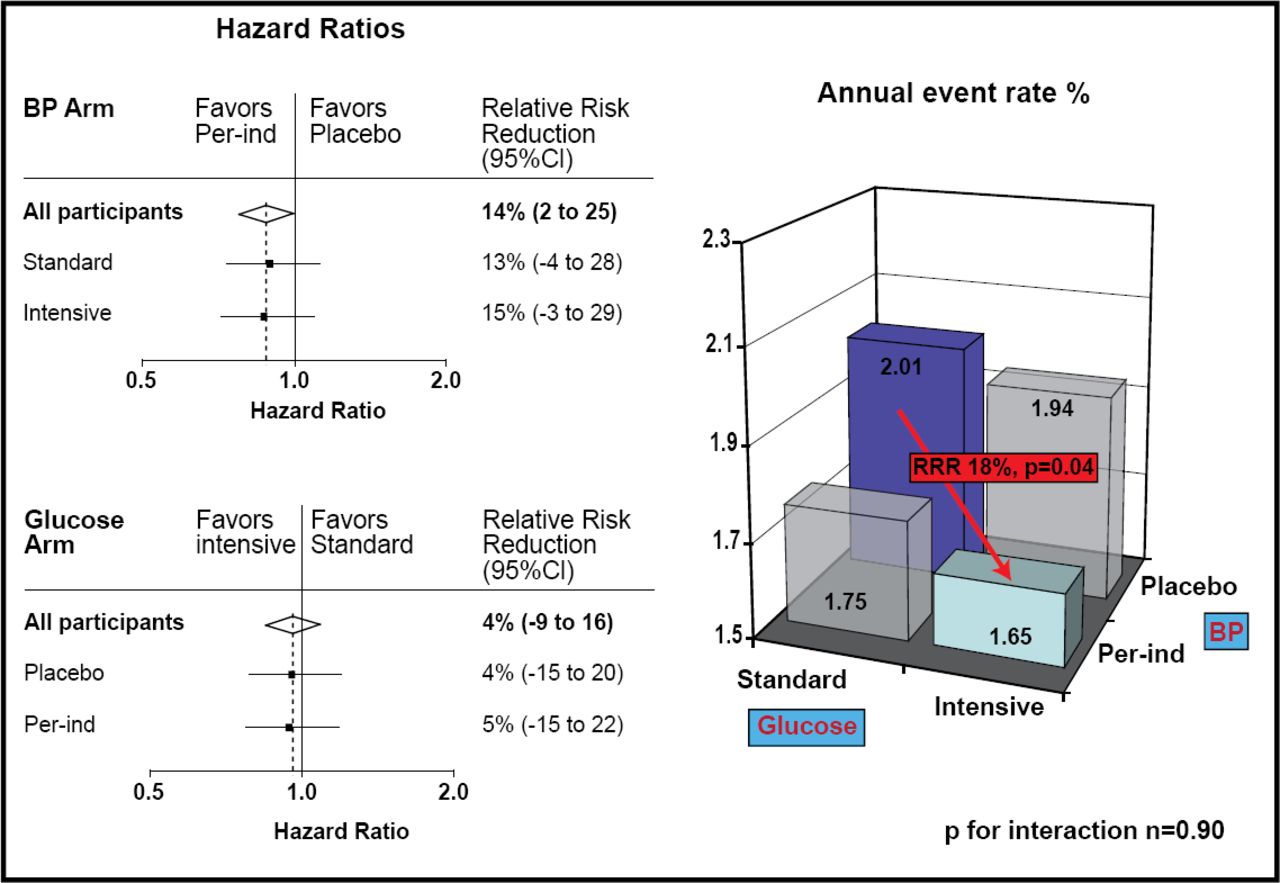
Further analysis of ADVANCE outcomes showed that the effects of blood pressure-lowering and intensive glucose control are independent, with no interaction between treatment approaches. In addition, the benefits of these treatment approaches are additive, leading to a greater reduction together than either strategy alone.
Compared with standard glucose control only, the combination of intensive glucose-lowering and blood pressure control reduced the annual risk of new or worsening nephropathy by 33% (p=0.005), reduced the risk of all-cause mortality by 18% (p=0.04; Figure 2), and reduced the risk of cardiovascular death by 24% (p=0.04). Given these clear benefits, the combined strategy of routine blood pressure-lowering and intensive glucose control is indicated for all patients with T2DM, Prof. Chalmers concluded.

Joint Effects of Blood Pressure Control and Intensive Glucose-Lowering on All-Cause Mortality.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.