

Summary
The medical advances of the last 30 years have been nothing less than astonishing; since 1970, there has been a 52% decrease in mortality from heart disease [Jemal A et al. JAMA 2005], and for the past decade, annual cancer deaths in the United States have fallen [Espy DK et al. Cancer 2007]. Thomas Insel, MD, Director, National Institute of Mental Health (NIMH), would like to extend the scope of these accomplishments to psychiatry.
- substance-related disorders
- mood disorders
- schizophrenia
- neurodevelopmental disorders
The medical advances of the last 30 years have been nothing less than astonishing; since 1970, there has been a 52% decrease in mortality from heart disease [Jemal A et al. JAMA 2005], and for the past decade, annual cancer deaths in the US have fallen [Espy DK et al. Cancer 2007]. Thomas Insel, MD, Director, National Institute of Mental Health (NIMH), would like to extend the scope of these accomplishments to psychiatry.
Consider the practice of medicine at large. In many ways, life is not as perilous as it once was; acute diseases, such as smallpox, are in sharp decline, and diseases that once were uncontrolled are now chronic, such as diabetes and hypertension. There is also movement toward personalized medicine. “We're moving from an era of ‘average’ medicine to a different kind of science—a way to tailor treatments to individual patients,” said Dr. Insel. This new way of thinking is well underway in oncology. Genetics is also having a continuing impact. The concept of Mendelian disease, in which pathology hinges on single, discrete mutations, such as in cystic fibrosis, is giving way to the reality that there often is a broad interplay of genes and regulatory pathways that are involved in a resulting pathologic phenotype. Again, cancer research largely has pointed the way. Dr. Insel proposes to apply these lessons to mental illness. “In our field, diagnosis is by observation—detection is late, and the ability to predict outcome poor. We know little about the causes of the most severe disorders,” he continued. Treatment largely is empirical, and no one is talking about cures. “I don't believe we have even the beginnings of research for a vaccine for schizophrenia or autism,” said Dr. Insel. “The bottom line is that neither prevalence nor mortality has decreased for any mental illness.”
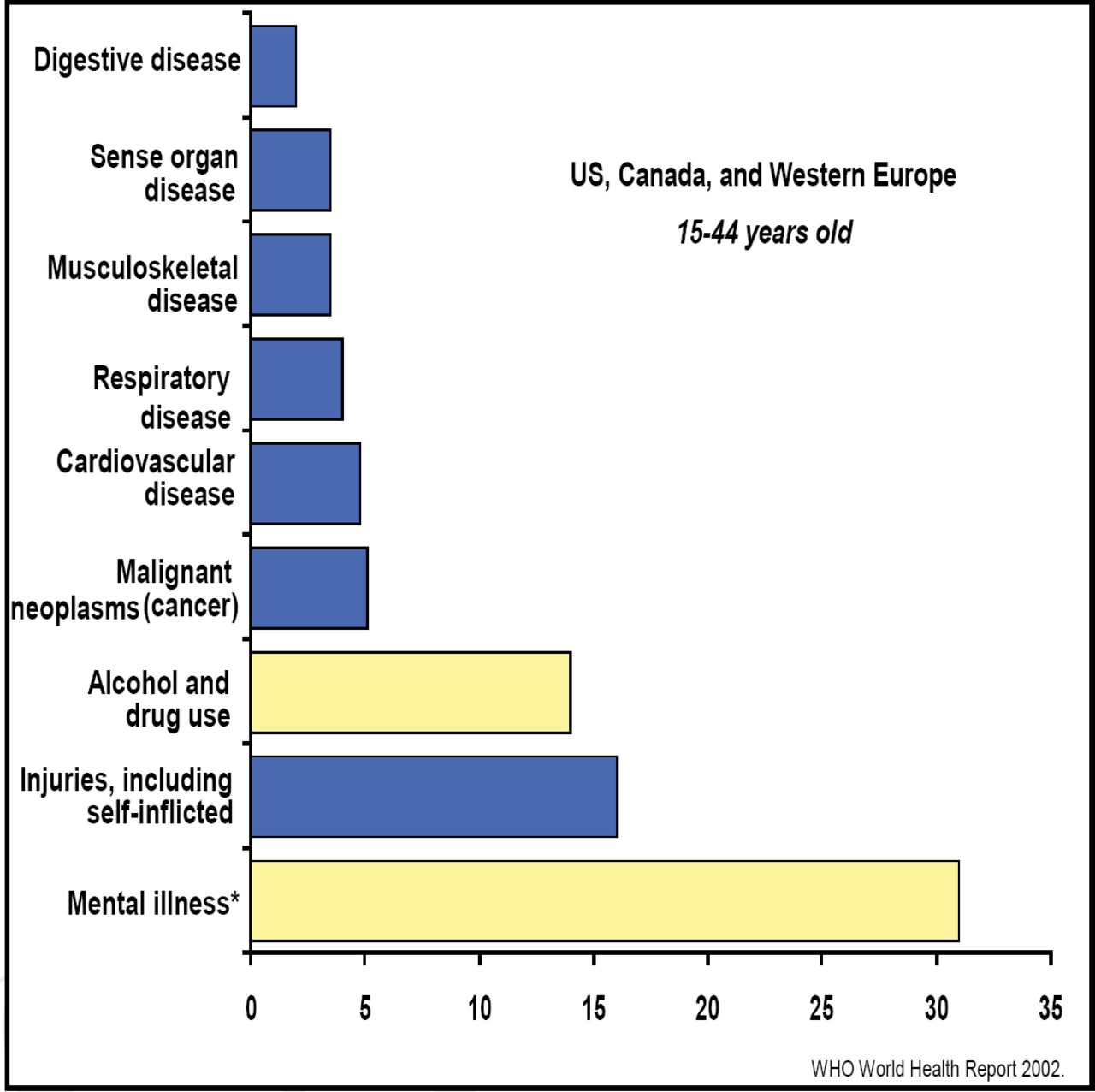
It's not as though research is lacking because psychiatric illnesses are rare. Mental disorders, including alcohol and drug addiction, account for half of the total disease burden in industrialized nations (Figure 1). In the US, it's estimated that 6% of the population has a disabling mental illness [Kessler RC et al. Arch Gen Psychiatry 2005], with over 28,000 related suicides (the annual rate for homicide is approximately 18,000 people per year; Conwell Y and Brent D. International Psychogeriatrics 1995; CDC Web-based Inquiry Statistics Query and Reporting System. www.cdc.gov.ncipc/wisqars/default.htm). Mental illness also precipitates physical illness, resulting in an average age at time of death of 56 years in this population [Colton CW, Manderscheid RW. Preventing Chronic Disease: Public Health Research, Practice and Policy 2006]. The need is clear. In order to enjoin the progress that has been seen in other disease states, Dr. Insel commends the broad adoption of 3 concepts that are now evolving in the field of psychiatry:
-
Mental disorders are brain disorders
-
Mental disorders are developmental disorders
-
Mental disorders result from complex genetic risk, plus experiential factors

Burden of Disease (DALYs).
Brain disorders
“Neurologists deal with dead cells—observable gross lesions. Psychiatrists deal with circuit problems,” said Dr. Insel. Only recently has the technology been available to image what is happening in brains of the mentally ill. Shaw and colleagues at the NIMH performed a brain imaging study of 223 children, aged 7–12 years, with diagnosed ADHD and 233 controls. Results showed a temporal deficit in cortical development in the ADHD children [Proc Natl Acad Sci 2007]. “These kids are about 3 years behind, developmentally,” said Insel. “ADHD can now be seen as a disease of cortical maturation—a brain disorder with cognitive and behavior manifestations.” This perspective immediately suggests a direction for treatment: Are cells not dividing? Do current medications have an impact on the maturation process? Already, there are new things to consider.
Depression also is yielding its physiologic secrets. Structural scans are elucidating dysfunction within the subgenual cingulate, also called Cg25, a region that is both reduced in volume and increased in activity in people with depression, some of which seems to be due to a reduction in glia [Nature 1997]. Data also show that when patients are treated for depression—irrespective of the methodology, pharmacotherapy or cognitive behavioral therapy (and even placebo)—there is a reduction in the metabolic activity in this region. “This is not the ‘home’ of depression,” Dr. Insel cautions. “It's a gateway. The important thing to remember is that this is a circuit problem. There are many ways into this circuit, suggesting new targets to treat depression.”
Developmental Disorders
The concept of mental disorders as developmental disorders is lost because the diagnosis tends to occur many years after the onset of symptoms. A recent study of adolescents looked at the epsilon4 allele of the ApoE gene—a risk factor for Alzheimer disease—and found that children who carried the risk allele already had a loss of cortical volume in the area that typically shows pathology at Alzheimer disease onset [Shaw P et al. Lancet Neurol 2007]. These children have no cognitive deficit, but these imaging findings suggest that a pathological process already is underway. Dr. Insel suggests a similar approach in schizophrenia by imaging those who exhibit the ‘prodrome,’ early characteristics of schizophrenia that precede psychosis [Arch Gen Psych 2008]. “For the last 20 years, we've been looking at schizophrenia as a disease that is defined by psychosis. I want to suggest to you that it's in this prodromal phase or even before the onset of the prodrome where we might have the best options for interventions with the greatest public health impact.”
Genetic Risk
The human genome contains millions of variations, large and small, which in aggregate may produce the phenotypes that are seen as psychopathology. Some of the same regions of variability appear to contribute to multiple, seemingly unrelated conditions; eg, Duchenne muscular dystrophy appears to involve some of the same genetic risk factors as common forms of heart disease, Crohn disease is related to certain cancers, and celiac disease shares genes with diabetes. “These are entirely new insights into pathophysiology,” said Dr. Insel. There are no reliable associations for mental disorders as yet, but the work is underway. “I suspect that we're going to have a very different impression of what many of these disorders are.” Yet, the value to be gained is not to provide a code for diagnosis, but a key to determining risk for a given patient, a pathway for discovering mechanisms of disease, and the possibility of developing preemptive treatments.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.