

Summary
Although a variety of treatments for major depression are available, less than 40% of patients achieve remission with their first treatment [Rush AJ et al. Am J Psychiatry 2006], and approximately 10% becomes treatment-resistant over time. New treatments are needed for patients who remain depressed despite having tried all available therapies. This article discusses the use of deep brain stimulation as a treatment for patients with chronic, treatment-resistant depression who have failed all other therapies.
- neuroimaging
- extrapyramidal & movement disorders
- mood disorders

Major depression is the most common of all psychiatric disorders [Wang PS. JAMA 2003] and the leading cause of disability in North America among adults under 50 years of age [World Health Organization 2001]. Although a variety of treatments are available, less than 40% of patients achieve remission with their first treatment [Rush AJ et al. Am J Psychiatry 2006], and approximately 10% becomes treatment-resistant over time. Although electroconvulsive therapy (ECT) is effective for many patients, those who have failed to respond to 4 previous antidepressant treatments are likely to relapse (CORE). New treatments are needed for patients who remain depressed despite having tried all available therapies.
Helen Mayberg, MD, Emory University, Atlanta, GA, has been investigating the use of deep brain stimulation (DBS) as a treatment for patients with chronic, treatment-resistant depression who have failed all other therapies. According to Dr. Mayberg, “It is now clear that depression cannot be viewed as simply a chemical “shortage” but rather as a more complex disorder of dysfunctional brain circuits.” The emerging evidence, made possible in large part by advances in imaging technology, indicates that depression is a “systems-level disorder affecting integrated pathways linking select cortical, subcortical, and limbic sites and their related neurotransmitter and molecular mediators” [Mayberg HS et al. Neuron 2005].
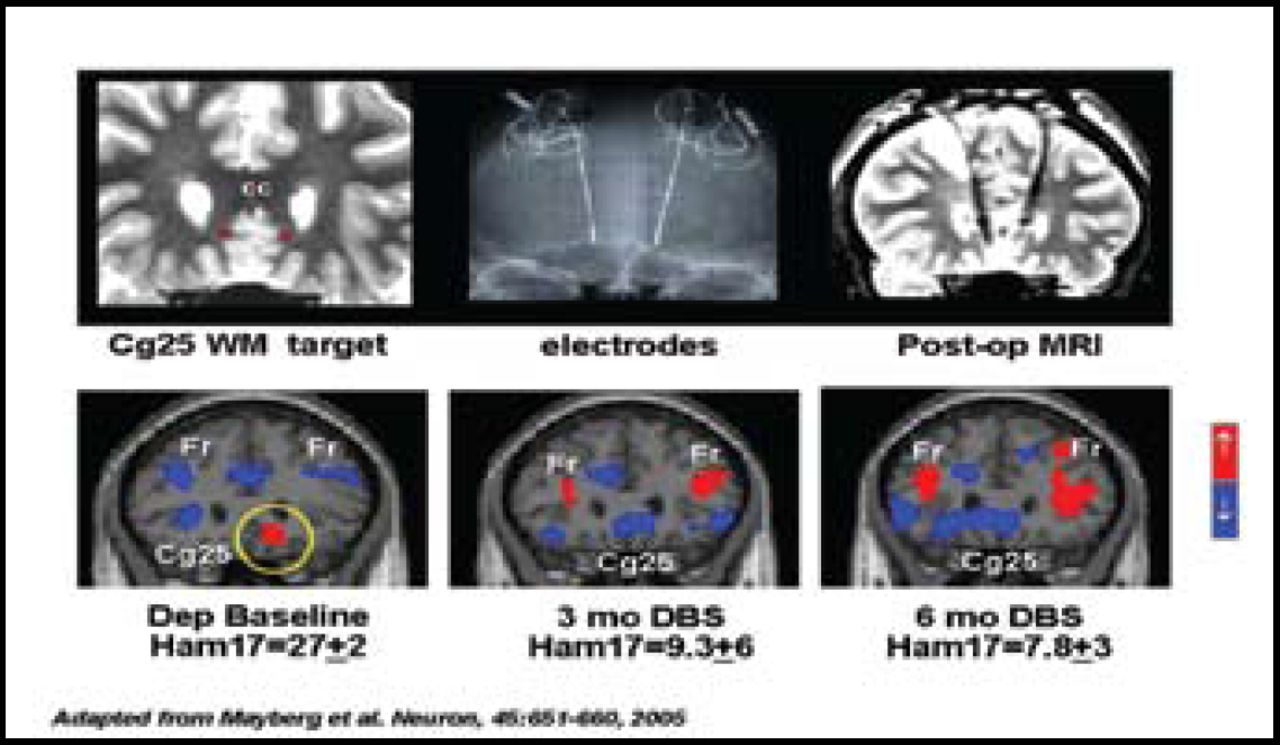
Although there are several circuits that might be targeted to produce clinical benefit in patients with treatment-resistant depression, Dr. Mayberg and her colleagues are particularly interested in the subgenual cingulate region of the brain (Cg25). Studies have indicated that Cg25 may play a role in modulating negative mood states [Mayberg HS et al. Am J Psychiatry 1999; Seminowicz DA et al. Neuroimage 2004], and a decrease in Cg25 activity has been shown in response to select SSRIs, ECT, repetitive transcranial magnetic stimulation (rTMS), and ablation [Mayberg HS et al. Neuron 2005]. It also has been suggested that certain Cg25 connections may be involved in the sleep, libido, appetite, and neuroendocrine disturbances that are associated with depression [Mayberg HS et al. Neuron 2005], as well as have an effect on other core behaviors that are affected by depression (eg, learning, memory, motivation, and reward).
The use of chronic high-frequency DBS has been shown to be effective in the treatment of Parkinson disease. Using that knowledge and evidence from worldwide studies that have shown that DBS produced local and remote changes in neural activity when applied to the basal ganglia, Dr. Mayberg and her colleagues continue to study the effect of DBS that is targeted to the Cg25 white matter of chronically depressed patients who do not respond to standard therapies.
DBS is accomplished using three-dimensional magnetic resonance imaging to guide the bilateral placement of very small wires deep into the brain. Patients are awake during this part of the procedure and have their skull secured in a special frame that allows very precise placement. The wires contain 4 contacts that span the areas to be stimulated. Once inserted, the contacts are tested to ensure that they are properly placed and to determine the appropriate level of stimulation. Following this, the patient is put to sleep, and the other end of the wire is connected to a small cable under the skin in the neck and then to a small battery pack. Ongoing stimulation is accomplished using a magnet and a small external control box (Figure 1).

Deep Brain Stimulation.
Photo courtesy of Medtronic.
In 2005, Dr. Mayberg and colleagues published the preliminary results of a pilot study of DBS in 6 patients with chronic, treatment-resistant depression [Mayberg HS et al. Neuron 2005]. In this study, patients showed progressive improvement over several weeks, and by 3 months, the investigators were able to distinguish between those patients who would go on to do well and those who would not. Four of the 6 patients achieved a good clinical result at 6 months (Figure 2). Follow-up continues on all patients, and the initial 4 responders continue to do well more than 4 years out with continuous DBS. As of 2008, 20 patients have received DBS implants as part of the original pilot study. Approximately 50 patients worldwide have been implanted in this same brain target, and placebo-controlled studies are now underway. Final results of the original 20-patient pilot project are now in press. Although these studies clearly offer hope to patients who have not responded to other treatments, Dr. Mayberg cautioned that “behavioral rehabilitation is still needed for patients after DBS.”

6-Month Results.
In closing Dr. Mayberg said, “The combination of deep brain stimulation and advanced imaging capabilities have given us new insights into the pathogenesis of depression that are laying the foundation for a whole new approach to the treatment of psychiatric disorders.”
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.