

Summary
This article discusses results from recent studies in 4 forms of empirically validated psychotherapy. Various topics include cognitive behavior therapy, behavior activation, interpersonal psychotherapy, and psychodynamic psychotherapy.
- mood disorders
Michael E. Thase, MD, University of Pennsylvania, Philadelphia, PA, discussed results from recent studies in 4 forms of empirically validated psychotherapy.
Cognitive Behavior Therapy (CBT)
“CBT is by far the most extensively studied of the 4,” said Dr. Thase. Recent studies include a trial from New Zealand that compared CBT with interpersonal psychotherapy (IPT) in 177 out-patients with major depressive disorder (MDD). Subjects received 8 to 19 therapy sessions over 16 weeks. The primary outcome was improvement in MADRS score. Although there was no difference in the 2 therapies on the primary outcome, results of a secondary analysis, conducted to determine the effect of personality disorder (PD) on both therapies, showed that PD did not adversely affect treatment response in patients who received CBT but did have an adverse affect on treatment response in those who received IPT [Joyce PF et al. Br J Psychiatry 2007].
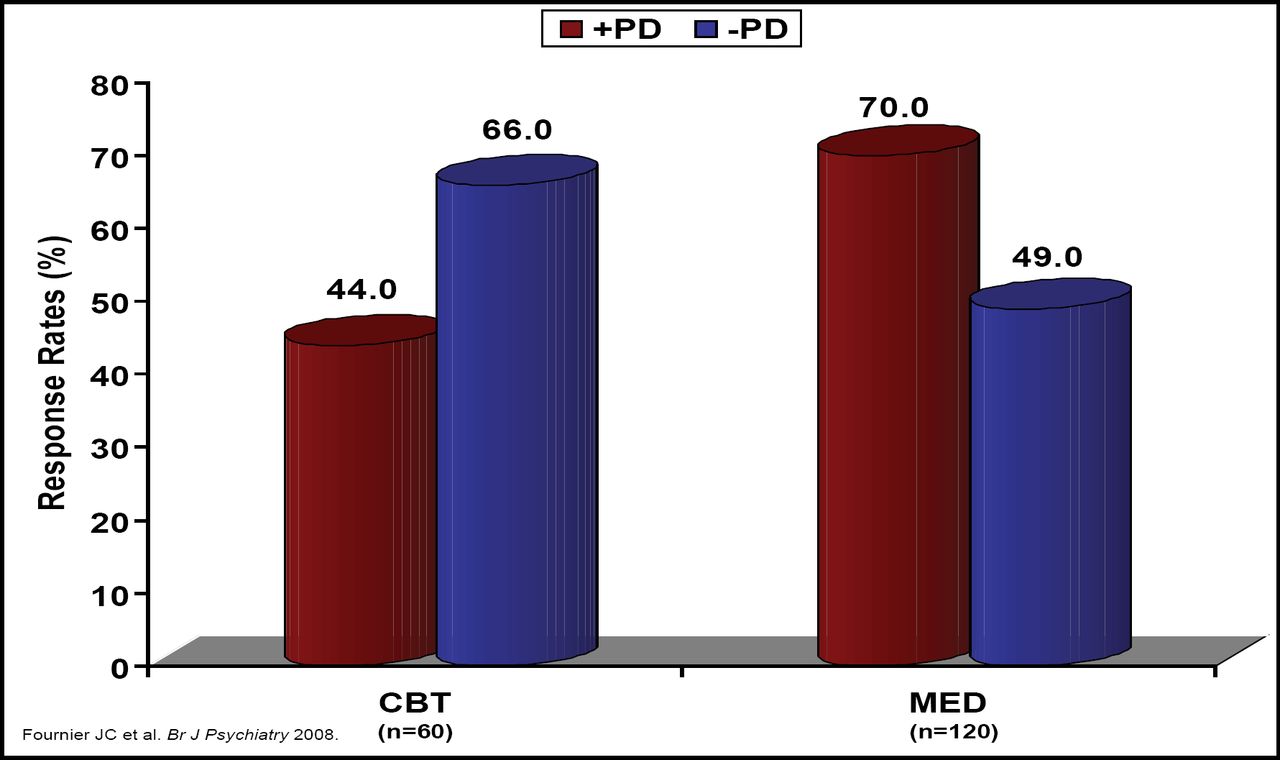
Although similar results concerning the effect of PD were seen in a sub-analysis from NIMH Treatment with Depression Collaborative study results, Fournier and colleagues found that while CBT was more than 20% better for the non-PD patients, pharmacotherapy was more than 20% better for the PD patients (Figure 1) [Fournier JC et al. Br J Psychiatry 2008]. “These conflicting results,” said Dr. Thase, “may indicate that in patients with significant PD, combination therapy might be the best option.”

Personality Disorder and Response Rates: CBT Versus Medication.
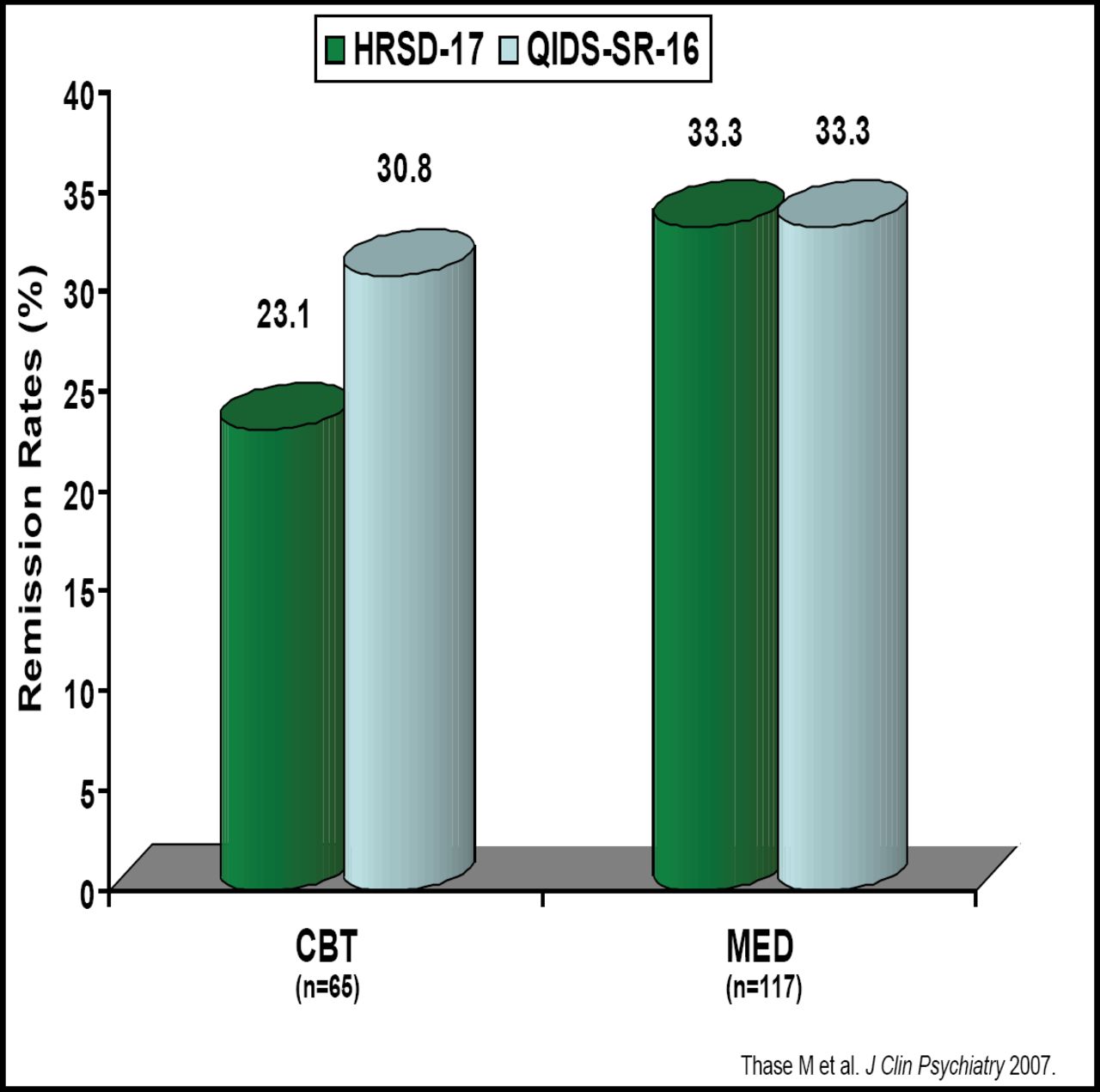
CBT also was evaluated in the STAR*D trial. Patients who did not benefit from citalopram alone were assigned to citalopram + CBT, citalopram + another antidepressant, CBT alone, or another antidepressant alone. Response and remission rates were similar between those who received any CBT and those who were assigned to medication alone; however, remission was significantly more rapid in subjects who received citalopram plus another medication versus those who received citalopram plus CBT (Figure 2) [Thase M et al. J Clin Psychiatry 2007].

Remission on CBT Versus Medication.
Behavior Activation (BA)
When Dimijian and colleagues compared the efficacy of BA versus CBT or antidepressant medication in a randomized, placebo-controlled trial in 241 adults with MDD, they found that among more severely depressed patients, BA was comparable with antidepressant medication and that both significantly outperformed CBT [Dimidjian S et al. J Consult Clin Psychol 2006].
However, a meta-analysis of 16 BA studies (including the Dimijian study) that comprised 780 subjects found no significant difference between BA and CBT. The differences between BA and cognitive therapy at follow-up also were non-significant [Cuijpers P et al. Clin Psychol Rev 2007] According to Dr. Thase, “Both of these studies show that BA is effective, and what is exciting about BA is that it is the kind of strategy that less sophisticated clinicians can learn to do and learn to do very quickly.”
Interpersonal Psychotherapy (IPT)
In one recent study, 124 moderate to severely depressed inpatients received either an intensive dose of individual and group IPT sessions along with pharmacotherapy or pharmacotherapy + clinical management. Patients received 15 individual sessions + 8 group sessions. The authors found that brief, intensive IPT was superior to standard treatment for these severely ill, hospitalized patients, and the differential effects lasted for 3 months [Schramm E et al. J Affect Disord 2007].
IPT does not appear to work in all patient populations. Results of a 12-week study in depressed patients who also had coronary artery disease (CAD) showed that IPT had no effect either alone or in combination, although citalopram did [Lespérance et al. JAMA 2007]. In addition, in a long-term study in older patients (>70 years) that evaluated whether maintenance antidepressant pharmacotherapy and IPT were able to sustain the health-related quality of life gains that were achieved during short-term treatment, Dombrovski found no benefit with IPT [Dombrovski AY et al. J Am Geriatr Soc 2007].
Psychodynamic Psychotherapy (PDP)
Until recently, there has been little scientific evidence that PDP has the same benefits as CBT or IPT. However, in a meta-analysis of 3 randomized, controlled trials that comprised 313 patients, de Maat and colleagues found that although medication combined with PDP was more effective than PDP alone, PDP alone was more effective than medication alone in treating depression [de Maat et al. in press].
In conclusion, Dr. Thase stated that, “We now have evidence from randomized, controlled trials that the modern depression-focused psychotherapies are effective for many patients with MDD. This is important, because if you don't use psychotherapy and focus primarily on pharmacotherapy, you are dealing with an incompletely effective modality of treatment. Of course, for the more-difficult-to-treat or the incompletely remitted patient, the additional benefit of using the 2 treatments in combination is an important and, in some ways, unique aspect that a psychiatrist can bring to treatment.”
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.