

Summary
This article discusses several meta-analyses that provide comparative safety data with respect to NSAIDs, as well as how to understand the data when interpreting NSAID risks, and balancing gastrointestinal and cardiovascular risks in patients requiring NSAIDs.
- arthritis
- rheumatoid arthritis
Understanding the Data: Interpreting NSAID Risks
Daniel Hal Solomon, MD, MPH, Brigham and Women's Hospital, Boston, MA, discussed several meta-analyses that provide comparative safety data with respect to NSAIDs.
In an analysis of data from randomized controlled trials (RCTs) that compared the risk for atherothrombosis with NSAIDs and COX-2 inhibitors, Kearney and colleagues found a similar, moderate increase in the overall incidence of serious vascular events for both therapies (1.0%/year vs 0.9%/year). However, a comparison of non-selective NSAIDs with placebo showed differences between NSAIDs, wherein naproxen was associated with the lowest risk (0.92; 95% CI, 0.67–1.21) [Kearney PM at al. BMJ 2006]. Results of another meta-analysis that compared results of studies that assessed cardiovascular (CV) events in patients who were treated with COX-2 inhibitors, NSAIDS, or both found a dose-related risk with rofecoxib (≤25 mg/day RR 1.33; 95% CI, 1.00–1.79; >25 mg/day RR 2.19; 95% CI, 1.64–2.91). Celecoxib was not associated with an elevated risk of vascular occlusion (RR 1.06; 95% CI, 0.91–1.23). Among NSAIDs, diclofenac had the highest risk (RR 1.40; 95% CI, 1.16–1.70). The relative risk with naproxen was 0.97 (95% CI, 0.87–1.07). The relative risk with ibuprofen was 1.07 (95% CI, 0.97–1.18) [McGettigan P et al. JAMA 2006].
Two RCTs that assessed CV risk were APC and MEDAL. The APC trial included 2035 subjects (mean age 60 years; 68% men; 30% taking aspirin) with prior colorectal adenoma. After 3 years of follow-up, there was a significantly (p=0.01) increased, dose-proportional risk with celecoxib (200 or 400 mg BID) versus placebo. Results of a subgroup analysis showed no impact on risk when analyzed for aspirin use, age, gender, CV risk factors, or diabetic status, although the data were underpowered for these subgroups [Solomon SD et al. N Engl J Med 2005]. In the MEDAL study (a pooled analysis of 3 randomized controlled trials in more than 34,000 osteo- and rheumatoid arthritis patients [mean age 63 years; 74% women] who were taking etoricoxib (60 or 90 mg/day) or diclofenac (75 mg BID), the hazard ratio for arterial thrombotic events for both drugs was close to 1 [Cannon CP et al. Lancet 2006].
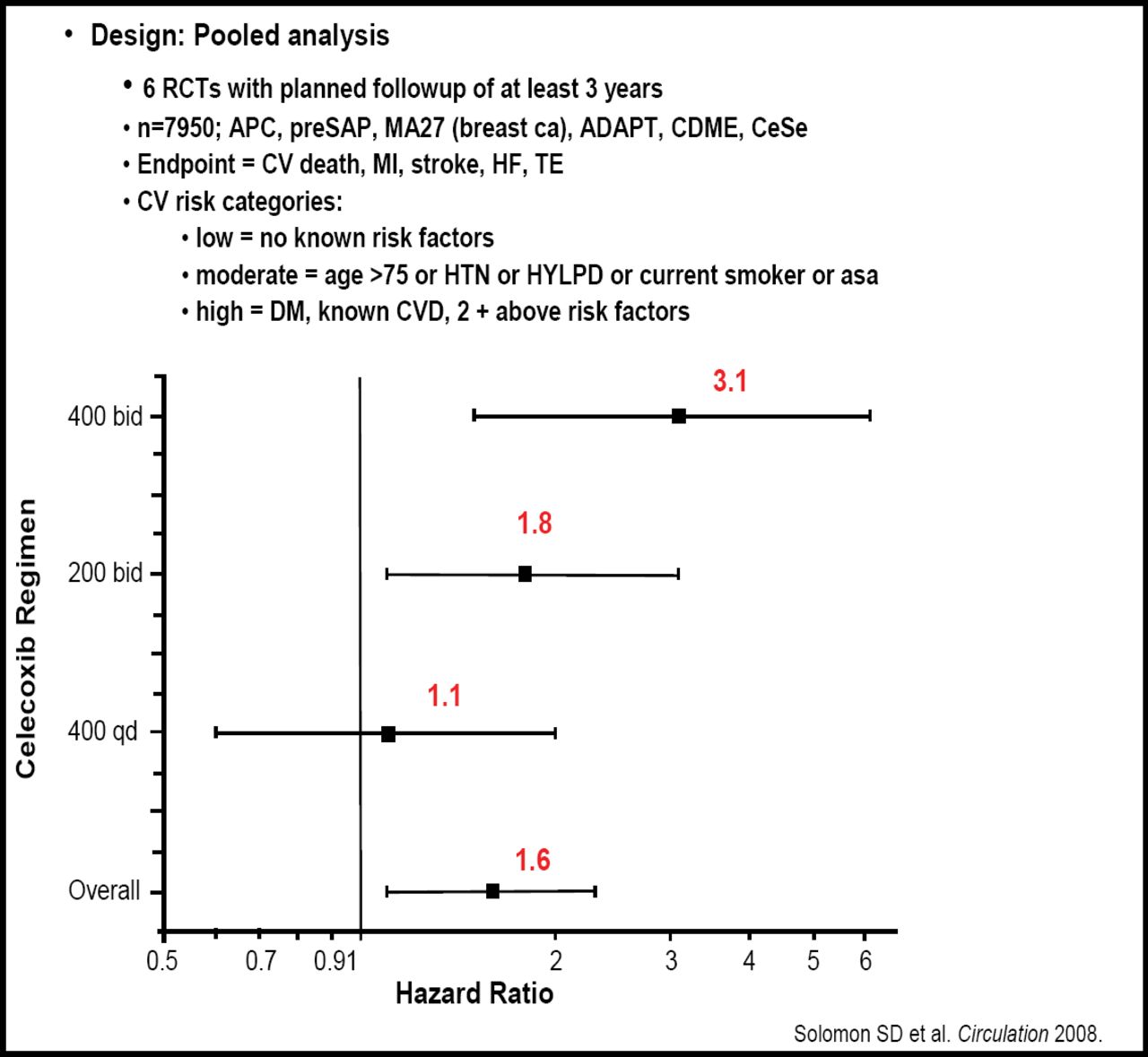
Scott D. Solomon, MD, Brigham and Women's Hospital, Boston, MA, and colleagues recently published the results of a pooled analysis of data from 7950 non-arthritis patients from 6 placebo-controlled trials that compared celecoxib (400 mg/day, 200 mg BID, or 400 mg BID) with placebo. The primary endpoint was the combination of CV death, myocardial infarction, stroke, heart failure, and thromboembolic event. With 16,070 patient-years of follow-up, the hazard ratio for the composite endpoint for all tested doses was 1.6 (95% CI, 1.1–2.3). Risk increased significantly across dose regimen (p=0.0005). Patients at highest baseline risk had a disproportionately greater risk of celecoxib-related adverse events (p for interaction=0.034; Figure 1) [Solomon SD et al. Circulation 2008].

Cross Trial Safety Assessment Group.
Balancing GI and CV Risks in Patients Requiring NSAIDs
NSAIDs are widely prescribed but can have serious gastrointestinal (GI) and CV side effects, which have led to the withdrawal of some of these drugs and continuing uncertainty about the best approach for patients who require NSAID therapy, particularly in those with GI or CV risk factors. Roger Jones, King's College London School of Medicine, London, UK, discussed results of a recently published review, which provides guidance on how to balance these risks in patients who require NSAIDs [Jones R et al. Am J Med 2008].
The damage to the GI tract that is caused by NSAIDs is the result of several factors, which include disruption of the protective mucus layer, inhibition of protective bicarbonate secretion, vasoconstriction (causing local tissue hypoxia), and superficial epithelial necrosis. NSAID injury occurs acutely in most patients who take aspirin and NSAIDs. Endoscopic studies indicate that 20% to 30% of regular NSAID users develop ulcers. Dyspepsia and heartburn occur in up to 60% of patients. The relative risk of developing clinically significant adverse events is 4.4 with concomitant use of corticosteroids at doses >10 mg/day and rises to 10.6 in patients aged over 75 years and to 12.7 in those who also use anticoagulants. Evidence from clinical studies indicates that CV events are a class effect of COX-2 inhibitors and that the most likely mechanisms are the effects of blood pressure elevation on endothelial function.
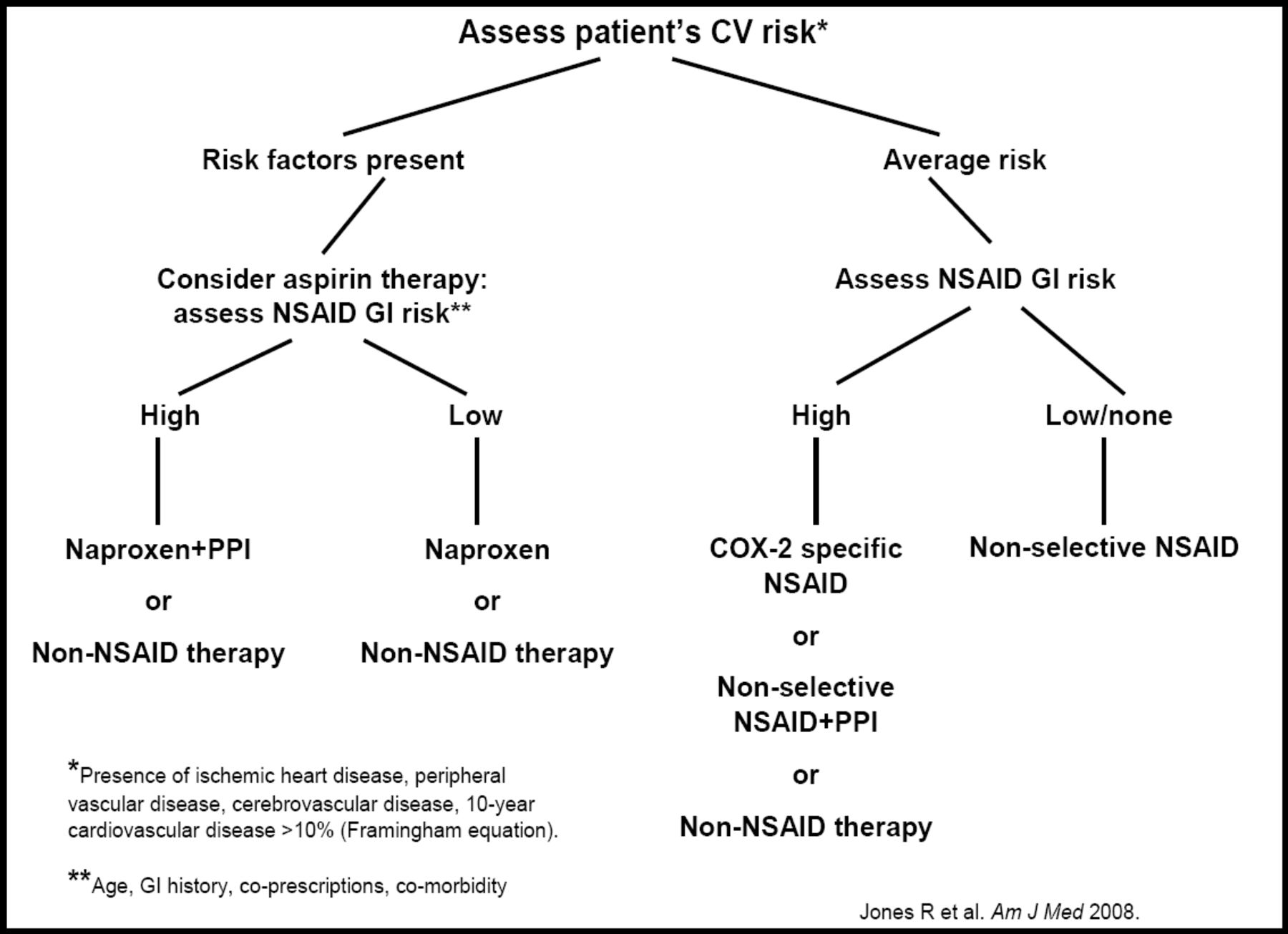
Although some key data are still lacking, Prof. Jones proposed the following recommendations with regard to treatment of patients who require NSAIDs (Figure 2):

Decision Tree for NSAID-Related Gastroprotection.
-
Avoidance of most NSAIDs (with the exception of naproxen) for patients with ischemic heart, cerebrovascular, or peripheral vascular disease, or a 10-year CV event risk ≥10%
-
COX-2 NSAIDs with/without gastroprotection for patients at increased risk of GI injury
-
Nonspecific NSAIDS (preferably naproxen) for patients who also require prophylactic low-dose aspirin, with consideration given to the addition of a gastroprotective agent for those at high risk for GI events
-
Naproxen monotherapy for patients without CV risk, who require aspirin prophylaxis for other reasons, and who are at low risk for GI events
-
COX-2 NSAID or a nonselective NSAID plus proton pump inhibitor for patients at risk of NSAID-related GI events, who do not require aspirin prophylaxis
-
Naproxen for patients taking aspirin, with consideration given to gastroprotection to reduce the risk associated with multiple NSAID therapy Prof. Jones cautioned that, “Physicians should pay attention to multiple and potentially competing factors in making a decision about NSAID prescription. While the challenge for the present is to balance their anti-inflammatory and analgesic actions against their many adverse effects, the challenge for the future is to develop equally efficacious drugs that do not share their side effect profiles.”
Prof. Jones cautioned that, “Physicians should pay attention to multiple and potentially competing factors in making a decision about NSAID prescription. While the challenge for the present is to balance their anti-inflammatory and analgesic actions against their many adverse effects, the challenge for the future is to develop equally efficacious drugs that do not share their side effect profiles.”
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.