

Summary
This article presents new data that affect the assessment and management of fibromyalgia. Advancements in our understanding of the biology of fibromyalgia have led to a variety of new treatment approaches. However, the need to use an evidence-based approach to the pharmacologic treatment of pain and fatigue, which are central complaints of patients who sufferfrom fibromyalgia.
- fibromyalgia
In this State-of-Art session, speakers presented new data that affect the assessment and management of fibromyalgia.
Advancements in our understanding of the biology of fibromyalgia have led to a variety of new treatment approaches. However, Leslie J. Crofford, MD, University of Kentucky, Lexington, KY, stressed the need to use an evidence-based approach to the pharmacologic treatment of pain and fatigue, which are central complaints of patients who sufferfrom fibromyalgia.
Significant to understanding the biology of chronic pain is the genetic basis for individual variations in pain perception. Diachenko and colleagues have identified 3 genetic variants (haplotypes) of the gene that encodes catecholamine-O-methyltransferase (COMT) that are associated with low, average, and high pain sensitivity [Diatchenko L et al. Hum Mol Genet 2005]. These haplotypes were shown to affect gene expression, norepinephrine concentrations, pain responsiveness, and risk of developing temporomandibular disorders (a chronic pain syndrome). It is certain that many more genes that affect the trait of pain sensitivity will be described and may lead to innovative treatments. Furthermore, recent data that concern the role of central sensitization of the pain system, impaired descending inhibitory pain pathways (abnormal pain processing within the central nervous system), and reduced availability of μ-opioid receptors in fibromyalgia patients have encouraged the testing of new treatment approaches that are focused on the central nervous system.
There are now 2 treatments that are approved for fibromyalgia in the United States, pregabalin and duloxetine. Pregabalin blunts the excess sensitivity of neurons by binding to ion channels. In the RELIEF and FREEDOM trials, pregabalin (300, 450, and 600 mg/day) produced significant improvement in endpoint mean pain score, sleep assessments, and patients' impressions of their global improvement, which was sustained over 6 months [Mease PJ et al. J Rheumatol 2008; Crofford LJ et al. Pain 2008].
The serotonin and norepinephrine reuptake inhibitors duloxetine and milnacipran (120 to 200 mg/day) have been shown to produce significant (p<0.05) reductions in pain, as well as improvements in global well-being, fatigue, and general functionality [Russell IJ et al. Pain 2008; Vitton O et al. Hum Psychopharmacol 2004; Gendreau RM et al. J Rheumatol 2005].
Prof. Crofford concluded with the following treatment recommendations: involve the patient in the treatment process; when evaluating progress, relate symptom (dominant) improvement to an increase in function; avoid the use of opioid analgesics, because they appear to be less effective in fibromyalgia patients; and be prepared to switch or combine treatments when one treatment approach does not seem to be effective.
Psychological Approaches to Management of Fibromyalgia
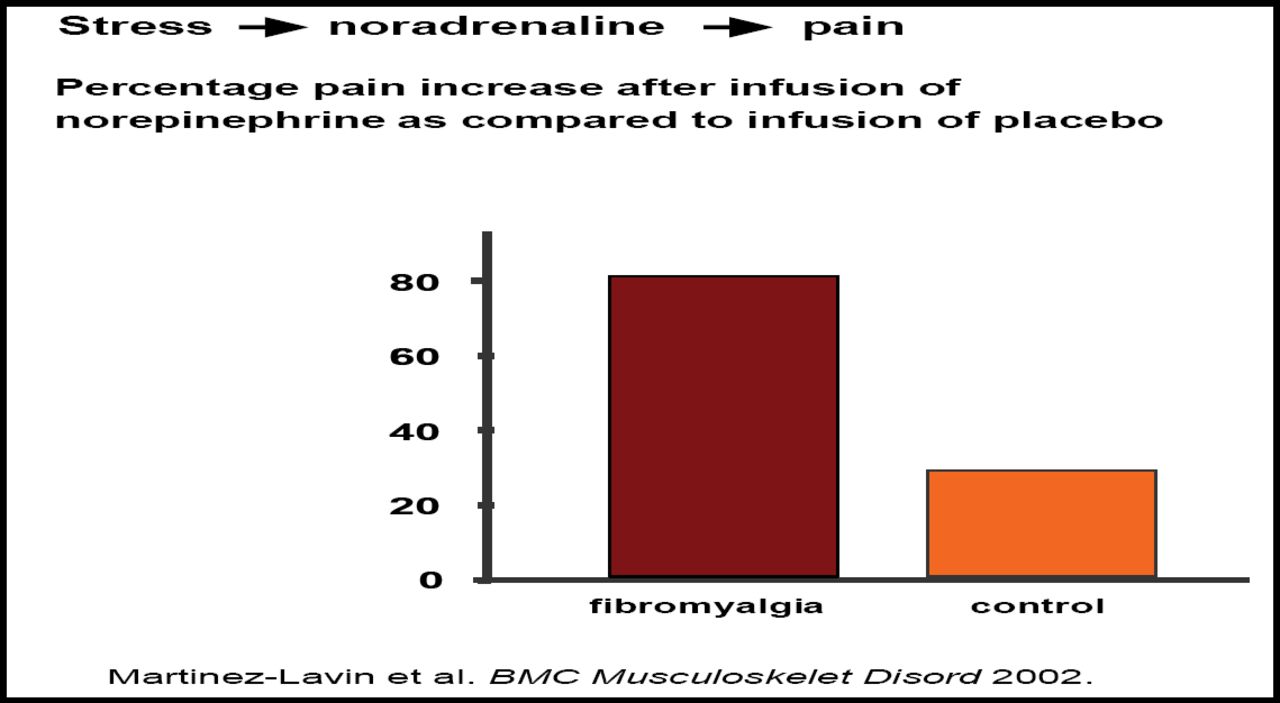
Rinie Geenen, PhD, Utrecht University, Utrecht, The Netherlands, presented evidence that indicated that psychological factors, such as stress and anger, and emotions in general, can amplify and mitigate pain; thus, psychological management of chronic pain as an adjunct to standard pharmacologic care may be useful. For instance, the intensity of norepinephrine-evoked pain is greater in fibromyalgia patients compared with rheumatoid arthritis patients and healthy controls (p<0.0001), which supports the hypothesis that fibromyalgia may be a sympathetically maintained pain syndrome that is amenable to psychological treatments [Martinez-Lavin M et al. BMC Musculoskelet Disord 2002] (Figure 1). Functional MRI biofeedback studies have demonstrated the ability of fibromyalgia patients to monitor and actively modulate areas of the brain (anterior cingulate cortex and right ventral prefrontal cortex) that are related to pain [de Charms RC et al. Proc Natl Acad Sci 2005].

Percentage of Pain Increase After Infusion of Norepinephrine as Compared to Infusion of Placebo.
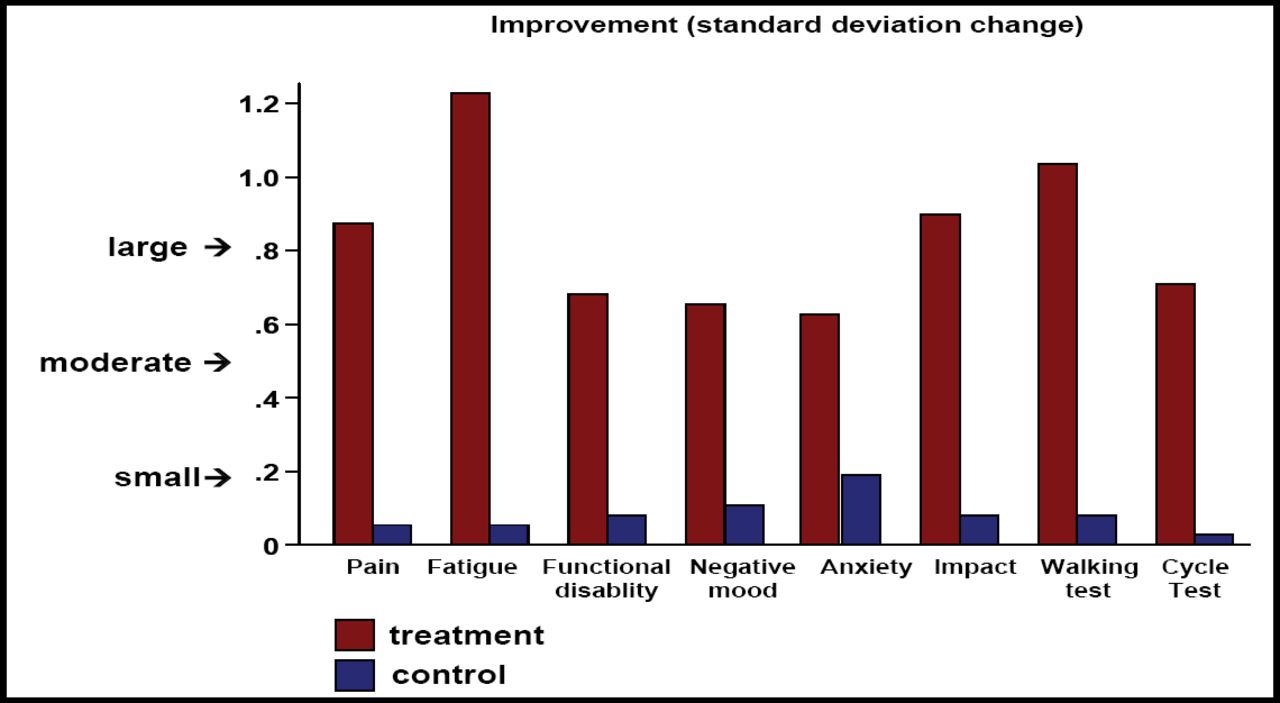
Prof. Geenen advocated and presented data to support the use of physical exercise training, cognitive-behavioral therapy, and education as interventions for fibromyalgia. Aerobic-only exercise training has been shown to have positive effects on global well-being and physical function, and possibly on pain and tender points [Busch AJ et al. Cochrane Database Syst Rev 2007]. Results from a recent (unpublished), randomized controlled trial that used tailored cognitive-behavioral therapy (CBT) composed of relaxation training, stress reduction, and management training, and pain and negative thought coping skills to treat fibromyalgia indicate moderate to large improvements in the areas of pain, fatigue, functional disability, negative mood, anxiety, and impact, as well as walking and cycling tests at post-treatment and the 6-month follow-up (Figure 2).

Effects of CBT in Treated Patients with Fibromyalgia as Compared to a Waiting-List Control Group.
Prof. Geenen concluded that there is accumulating evidence that the non-pharmacologic management of chronic pain as an adjunct to standard pharmacologic treatment offers significant benefits.
Do We Need New Diagnostic Criteria for Fibromyalgia?
The 1990 guidance for the classification of fibromyalgia syndrome has 2 criteria: a history of chronic, widespread pain and presence of 11 of 18 tender point sites on digital palpation. Although the criteria have made a significant contribution to research and clinical recognition of the condition, Ernest Choy, MD, Kings College, London, UK, suggested that recent evidence of deficiencies argues strongly for new diagnostic criteria that can assist clinicians in making a diagnosis of fibromyalgia and help to reduce the health care burden of the illness. In support of the latter, he listed the following symptoms—fatigue, sleep disturbance, headache, subjective joint swelling, morning stiffness, paraesthesia, IBS, dysmenorrhoea, anxiety, depression, failure to cope, poor self-reported state of health, poor self-reported physical function, and poor emotional function—noting that patients report experiencing an average of 6–11 of these symptoms, most of which are rated as very or extremely disruptive; yet, the current ACR criteria did not include the multi-symptomatic nature of the disease. Hence, Prof. Choy believes that the number of domains in the current ACR criteria do not adequately reflect the symptoms of fibromyalgia. The heterogeneity of the symptom profile among patients with fibromyalgia suggests a difference in the relative contributions of biologic, psychologic, and cognitive factors in individual patients. Three subgroups have been identified. One exhibits moderate levels of anxiety, depression, and poor pain control but the highest pain thresholds and low tenderness. The second subgroup encompasses those with high levels of anxiety, depression, and catastrophizing; low pain control; and considerable tenderness, whereas the third has low levels of anxiety, depression, and catastrophizing; good pain control; but very low pain thresholds and the most tenderness [Giesecke T et al. Arthritis Rheum 2003]. The issue of subgroups is not addressed by the ACR criteria.
Furthermore, a recent study that compared different approaches in diagnosing fibromyalgia—ACR criteria, clinician diagnosis, and survey diagnosis—found only a moderate degree of agreement. Importantly, the use of 11 of 18 tender points was insensitive. Interestingly, using 6 tender points at a cutoff would increase sensitivity without significantly compromising specificity. There is significant evidence based on functional neuroimaging that abnormal pain processing is the central pathophysiology in fibromyalgia. Objective tools need to be developed to assess pain processing in fibromyalgia.
Prof. Choy and other colleagues are in the process of developing new classification criteria for fibromyalgia syndrome.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.